THIS IS JUST A VERY GREATLY ABBREVIATED LIST OF VACCINE INJURIES COMPILED BY K.C. SHE HAS LISTS AND LISTS OF ARTICLES AND STUDIES TO BACKUP HER WORK.
GO TO THE LINK TO PERUSE THEM ALL: https://ladycasey.substack.com/p/scientific-studies-on-vaccine-injuries?utm_source=substack&utm_campaign=post_embed&utm_medium=email
This post mainly consists of scientific studies (both peer reviewed and preprints), systematic reviews, case studies (a few key ones of the thousands out there), and other medical journal articles that support the assertions in my Vaccine Injury post from November 2022. I began bookmarking these studies in late 2021, but since I’ve surely missed some, this is not a comprehensive list. It is, however, significant enough to utterly debunk the “safe and effective” propaganda of the past three years. (I will continue adding to this list indefinitely, so please check back on occasion for the most recent scientific discoveries about C19 vaccine injuries.)
I’m not a scientific researcher, data analyst, or medical professional. Neither are most of my readers. However I, and presumably they/you, are fully intellectually capable of reading and understanding the discussions and conclusions in most of the studies listed below. For those of you who prefer to skim, in most cases, after each link below, I include a short (2-3 sentence) summary of the study’s conclusions.
Some of the studies below are followed by a supporting article explaining its findings in layman’s terms. All such articles are written by experts in their field, including scientific researchers, professors, data analysts, PhDs, MDs and other medical professionals. (Some accompanying articles are under a paywall, for which I apologize, however I’m happy to email my readers free versions of any linked articles upon request.)
Lastly, please take note that much of the pro-jab jargon used in these studies is required to survive peer review. Journals are beholden to (funded and captured by) the pharmaceutical industry. Researchers have stated outright that they cannot get published on this topic without the inclusion of pro-vaccine rhetoric in their studies.
Please use this post as a resource to backup your own arguments with uninformed acquaintances who continue to believe and perpetuate the false government/Pharma narrative that the C19 “vaccines” are safe. They are not, and the following evidence couldn’t be more clear about that.
General Adverse Events
Serious Adverse Events of Special Interest Following mRNA Vaccination in Randomized Trials https://www.sciencedirect.com/science/article/pii/S0264410X22010283
(Peter Doshi—senior editor of the BMJ—study concluding that Covid vaccines were associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated. And that the excess risk of serious adverse events of special interest surpassed the risk reduction for COVID-19 hospitalization. Explanatory articles here, here, and here.)
COVID-19 Modified mRNA “Vaccines” Part 1: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex https://www.ijvtpr.com/index.php/IJVTPR/article/view/101
(“The usual safety testing protocols and toxicology requirements were bypassed. Many key trial findings were either misreported or omitted entirely from published trial reports. By implication, the secondary estimates of excess morbidity and mortality in both trials must be deemed underestimates. Rigorous re-analyses of trial data and post-marketing surveillance studies indicate a substantial degree of modmRNA-related harms than was initially reported. Confidential Pfizer documents had revealed 1.6 million adverse events by August 2022. A third were serious injuries to cardiovascular, neurological, thrombotic, immunological, and reproductive systems, along with an alarming increase in cancers. Moreover, well-designed studies have shown that repeated modmRNA injections cause immune dysfunction, thereby potentially contributing to heightened susceptibility to SARS-CoV-2 infections and increased risks of COVID-19. This paper also discusses the insidious influence of the Bio-Pharmaceutical Complex, a closely coordinated collaboration between public health organizations, pharmaceutical companies, and regulatory agencies.” Read the original paper here and explanation of its highly suspect & unethical redaction here.)
Potential health risks of mRNA-based vaccine therapy: A hypothesis https://www.sciencedirect.com/science/article/pii/S0306987723000117
(“If our hypothesis were to be confirmed, the implications for public health would be staggering and appalling in the context of the mass-scale COVID-19 vaccination already taking place, particularly if the nms-mRNA enters brain, bone marrow, and – if already present in the vaccinee – cancerous or pre-cancerous cells, or if the vaccine is administered to females early in their pregnancy and the nms-mRNA transfects embryonic cells.”)
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA https://www.mdpi.com/2227-9059/11/8/2287
(“This paper reviews autoimmune, cardiovascular, neurological, potential oncological effects, and autopsy evidence for spikeopathy.” Also, ” Treatment modalities for ‘spikeopathy’-related pathology in many organ systems, require urgent research and provision to millions of sufferers of long-term COVID-19 vaccine injuries. We also advocate for the suspension of gene-based COVID-19 vaccines and lipid-nanoparticle carrier matrices, and other vaccines based on mRNA or viral-vector DNA technology.” Comprehensive explanatory article here.)
The Novelty of mRNA Viral Vaccines and Potential Harms: A Scoping Review https://www.mdpi.com/2571-8800/6/2/17
(The COVID-19 vaccines are known to be unsafe for several reasons: 1) the Wuhan Spike protein damages cells, tissues, organs, and causes blood clotting, 2) the lipid nanoparticles may have toxicity from the PEG or polysorbate 80 or from syncytia formation, 3) the mRNA appears to be resistant to ribonucleases and is not broken down in the body. As some point the mRNA or fragments could interfere with gene function or alter other microRNAs that are managing the human genome. Explanatory article here.)
When the county’s death data is applied nationwide, researchers estimate 49,240 Americans died from vaccine-induced cardiopulmonary arrest.
A study co-authored by Dr. Peter McCullough, published Monday, has found that there was a 1,236 percent increase in death in King County, Washington between 2020 and 2023. The county has a high rate of vaccination, as 98 percent of its residents received at least one Covid injection by 2023.
“Our analysis revealed a 25.7% increase in total cardiopulmonary arrests and a 25.4% increase in cardiopulmonary arrest mortality from 2020 to 2023 in King County, WA. Excess cardiopulmonary arrest deaths were estimated to have increased by 1,236% from 2020 to 2023, rising from 11 excess deaths (95% CI: -12, 34) in 2020 to 147 excess deaths (95% CI: 123, 170) in 2023. A quadratic increase in excess cardiopulmonary arrest mortality was observed with higher COVID-19 vaccination rates,” the study said in the ‘Results’ section.
The researchers also collected data from emergency medical services (EMS) reports, the U.S. Census Bureau and The Tennessean COVID-19 Vaccine Tracker in order to apply their findings from King County to the wider American population.
“The excess mortality model for King County was used to calculate yearly estimates for excess cardiopulmonary arrest fatalities in the USA,” the study said in the ‘Methods’ section.
“Applying our model from these data to the entire United States yielded 49,240 excess fatal cardiopulmonary arrests from 2021-2023,” the study said in the ‘Results’ section.
URGENT! Keep Alex Jones in the fight against the NWO! Please pray & contribute at DefendJones.com today!
The researchers concluded by giving their opinion on the findings and documenting why the death rate increase is attributed to the Covid injections.
“The biological plausibility of death from acute cardiac and pulmonary causes after COVID-19 vaccination has been previously demonstrated and is concerning given these real-world observations. Urgent further research is needed to determine if similar trends are observed in other regions with attention to risk mitigation for incident events and improved survival with resuscitation,” the study said in the ‘Conclusions’ section.
The CDC recommends all Americans receive their Covid shot and that young children receive extra, while Canada recommends another Covid shot for the pregnant, indigenous, ‘racialized’ & ‘equity-deserving’.
The FAA quietly widened the EKG parameters beyond the normal range (from a PR max of .2 to unlimited) in its Guide for Aviation Medical Examiners in October 2022. It was done after the vaccine rollout. Kirsch says this is a tacit admission from the US government that the COVID vaccine has damaged the hearts of American pilots. Kirsch believes the actual rate of heart injury from COVID vaccines is well over 29.7%, based on a study from Thailand. He wrote that at a 20% injury rate, 50 million Americans have heart damage caused by the jab. He stated that nursing homes have lost up to 33% of their residents in 12 months where before they were losing only 1 or 2% a year.
In the October 2022 version of the FAA Guide for Aviation Medical Examiners, the FAA quietly widened the EKG parameters beyond the normal range (from a PR max of .2 to unlimited). And they didn’t widen the range by a little. They widened it by a lot. It was done after the vaccine rollout.
This is extraordinary. They did it hoping nobody would notice. It worked for a while. Nobody caught it.
But you can’t hide these things for long.
This is a tacit admission from the US government that the COVID vaccine has damaged the hearts of our pilots. Not just a few pilots. A lot of pilots and a lot of damage.
The cardiac harm of course is not limited to pilots.
My best guess right now is that over 50M Americans sustained some amount of heart damage from the shot.
That’s a lot of people who will be very upset when they realize the vaccine they took to reduce their chance of dying from COVID actually worked in reverse making it:
More likely that people will get COVID
Be hospitalized from COVID and other diseases
Die from COVID (and other diseases)
You also have an excellent chance of getting a lifetime of heart damage for no extra charge.
But don’t worry; you can’t sue them. They fixed the law so none of them aren’t liable (the doctors, the drug companies, the government). After all, you took the vaccine of your own free will. It’s not like you were forced (or coerced) to take it or anything like that! And there were plenty of people warning you not to take the shots (even though they censored most of them).
In this article, I will explain the evidence and thinking behind all my claims.
As I learn more, I will refine the estimate.
Introduction
On October 24, 2022, the FAA quietly, without any announcement at all, widened the EKG requirements necessary for pilots to be able to fly.
The PR (a measure of heart function) used to be in the range of .12 to .2.
It is now: .12 to .3 and potentially even higher.
This is a very wide range; it accommodates people who have cardiac injury. Cardiologist Thomas Levy is appalled at this change:
Save
Why did they make the change?
Why would they do that?
I’ll take an educated guess as to why they did that. I believe it is because they knew if they kept the original range, too many pilots would have to be grounded. That would be extremely problematic; commercial aviation in the US would be severely disrupted.
And why did they do that quietly without notifying the public or the mainstream media?
I’m pretty sure they won’t tell me, so I’ll speculate: it’s because they didn’t want anyone to know.
In other words, the COVID vaccine has seriously injured a lot of pilots and the FAA knows it and said nothing because that would tip off the country that the vaccines are unsafe. And you aren’t allowed to do that.
Why we sure it was the vaccine that did it
There are several clues that are consistent with “it was the vaccine and not COVID”:
They were quiet about it. If it was COVID, you can be public. But the vaccine is supposed to be safe.
The timing. October 2022 is late for COVID. If it was due to COVID, it would have happened well before now. They can make changes every month.
The vaccine creates far more injury to the heart than COVID (which creates NO added risk per this large-scale Israeli study of 196,992 unvaccinated adults after Covid infection).
Anecdotally, cardiologists only started to notice the damage post-vaccine.
There was a study done on pilots. It will be published in The Epoch Times later this week. That indicated heart damage in over 20% of pilots screened (The Epoch Times will release the exact number).
The Thailand study showed nearly 30% of kids were injured. But kids are indestructible so a 30% injury rate in kids translates into a higher rate for adults.
VAERS shows that cardiac damage happens at all ages, not just the young:
Save
Bottom line: The most logical conclusion is that the FAA knows the hearts of our nations pilots have been injured by the COVID vaccine that they were coerced into taking, the number of pilots affected is huge, the cardiac damage is extensive, and passenger safety is being compromised by the lowering of the standards to enable pilots to fly.
The right thing would be for the FAA to come clean and admit to the American public that the COVID vaccine has injured 20% or more of the pilots (based on their limited EKG screening), but I doubt that they will ever do that.
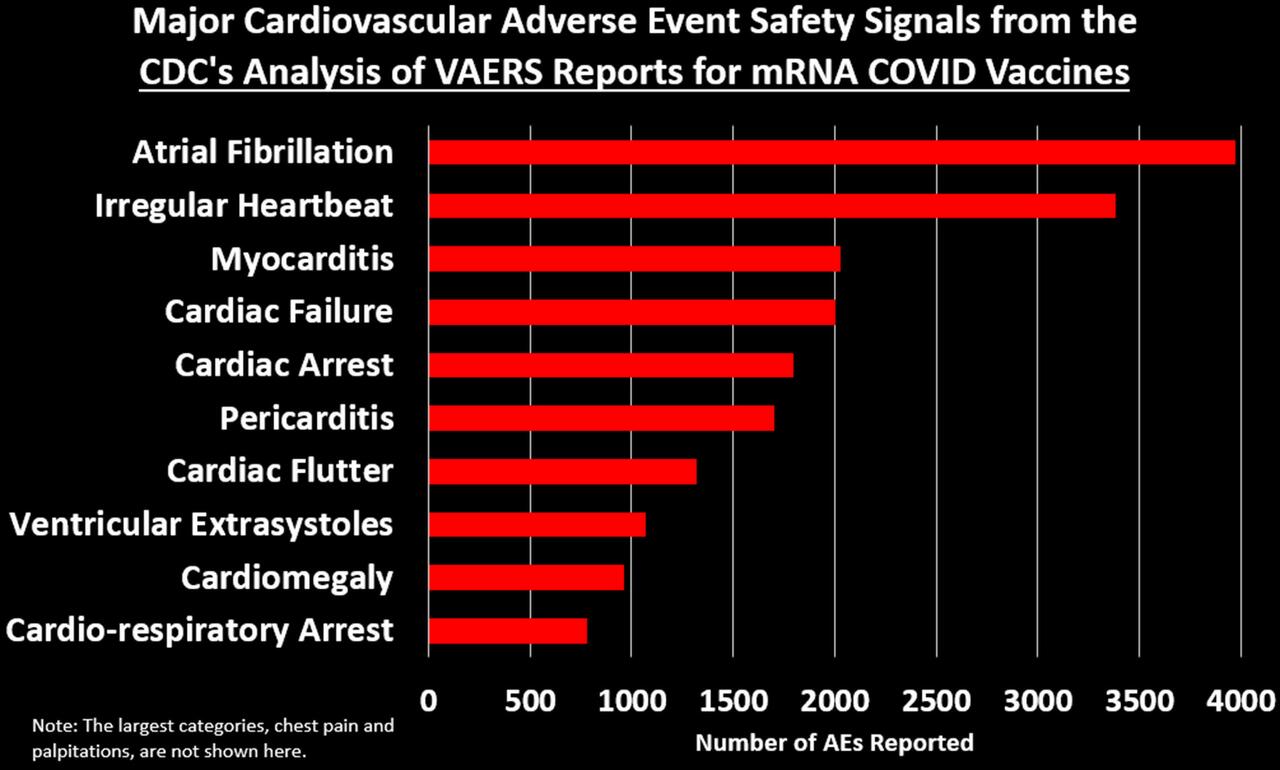
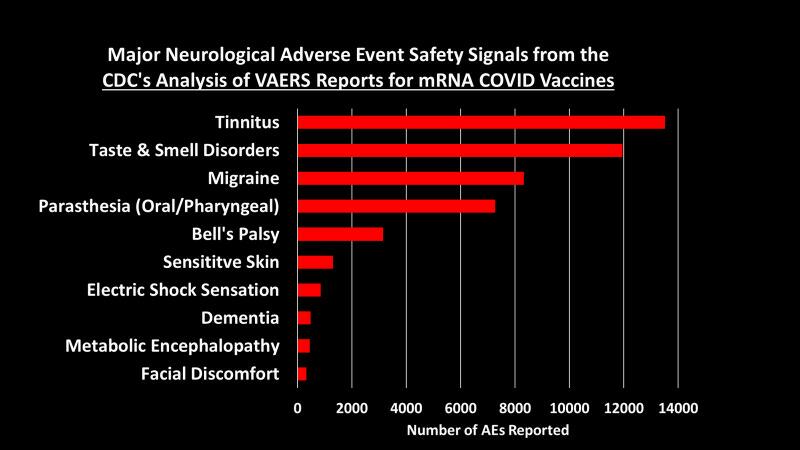
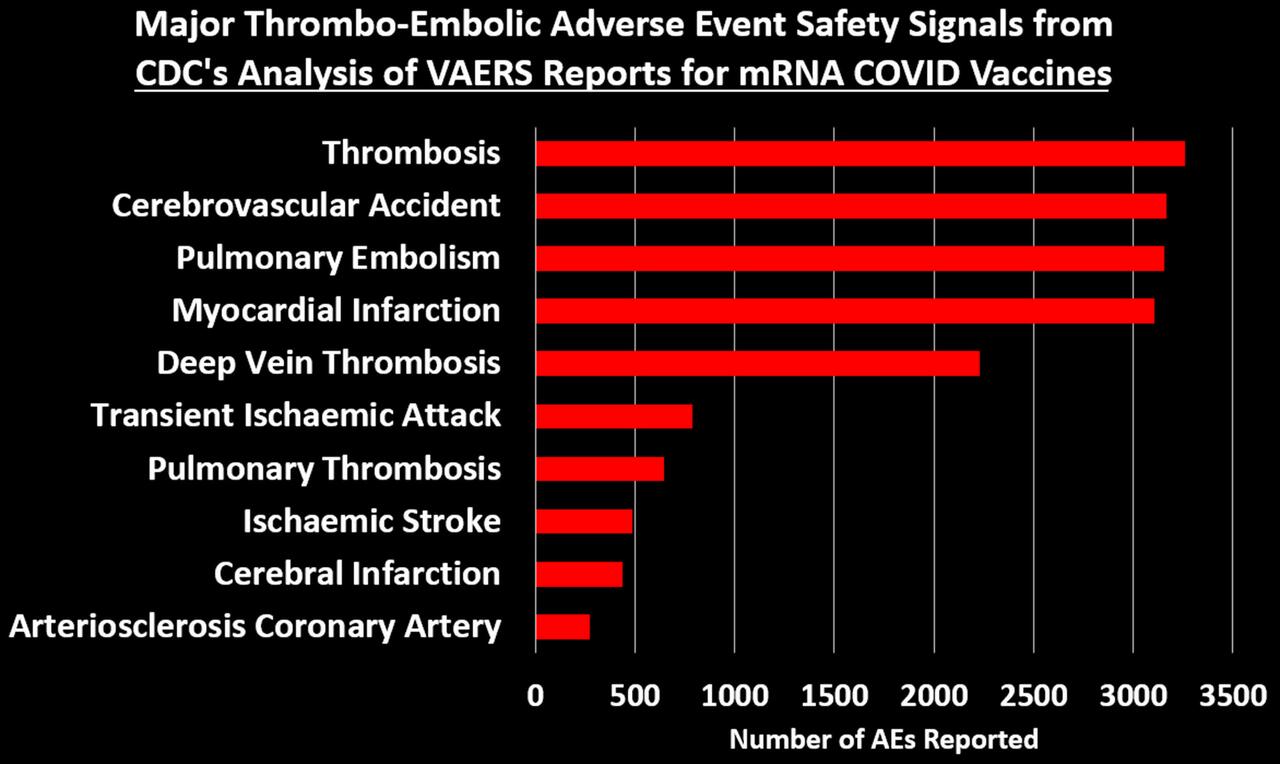
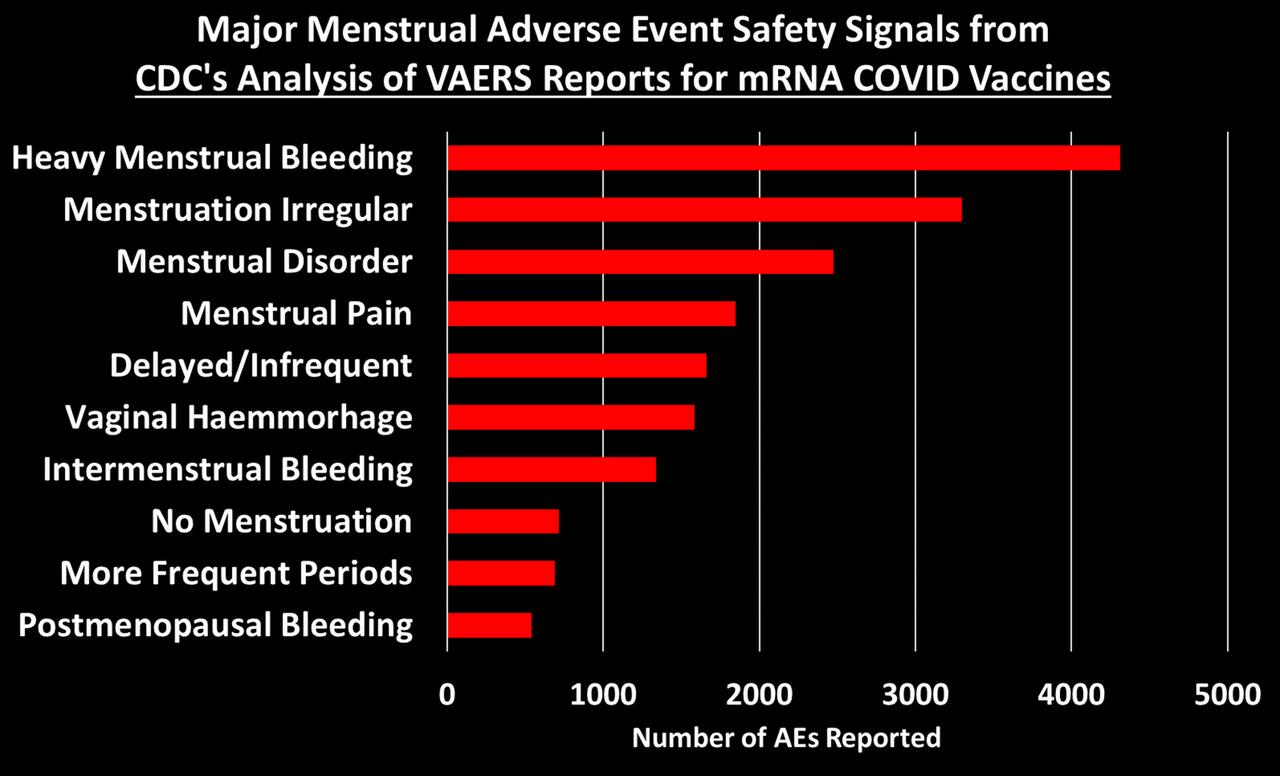
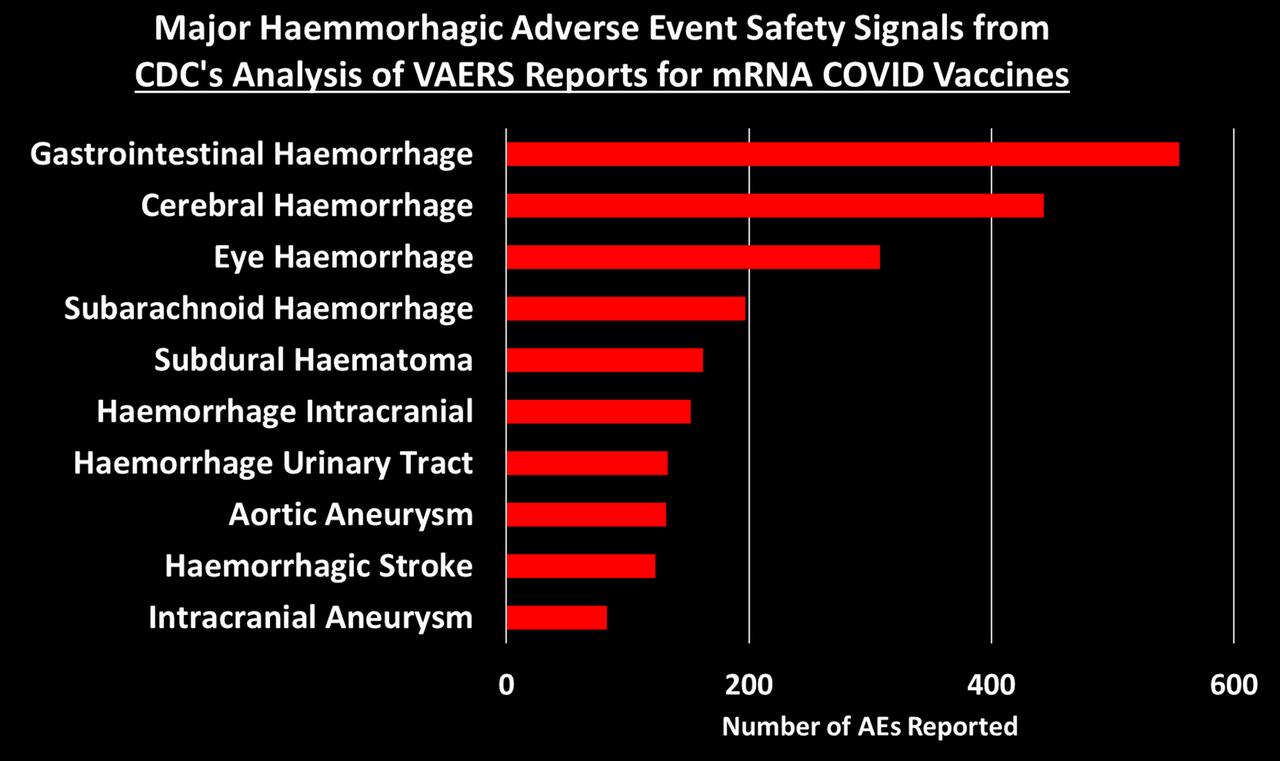
CDC’s VAERS safety signal analysis based on reports from Dec. 14, 2020 – July 29, 2022 for mRNA COVID-19 vaccines shows clear safety signals for death and a range of highly concerning thrombo-embolic, cardiac, neurological, hemorrhagic, hematological, immune-system and menstrual adverse events (AEs) among U.S. adults.
There were 770 different types of adverse events that showed safety signals in ages 18+, of which over 500 (or 2/3) had a larger safety signal than myocarditis/pericarditis.
The CDC analysis shows that the number of serious adverse events reported in less than two years for mRNA COVID-19 vaccines is 5.5 times larger than all serious reports for vaccines given to adults in the US since 2009 (~73,000 vs. ~13,000).
Twice as many mRNA COVID-19 vaccine reports were classified as serious compared to all other vaccines given to adults (11% vs. 5.5%). This meets the CDC definition of a safety signal.
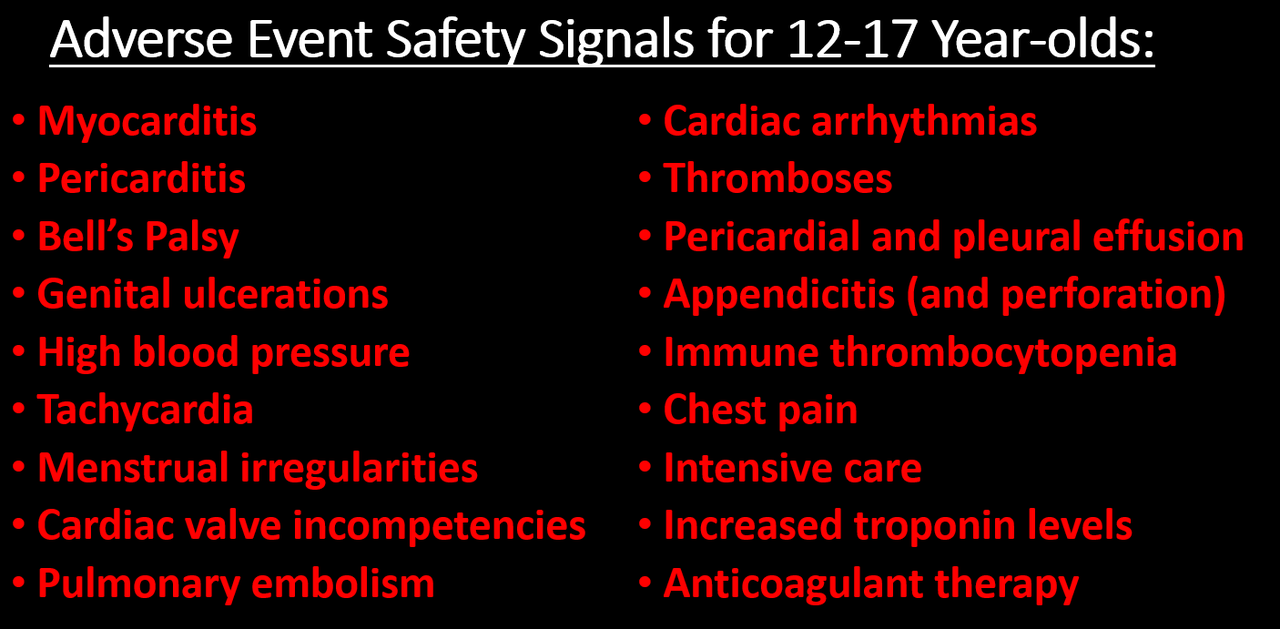
There are 96 safety signals for 12-17 year-olds, which include: myocarditis, pericarditis, Bell’s Palsy, genital ulcerations, high blood pressure and heartrate, menstrual irregularities, cardiac valve incompetencies, pulmonary embolism, cardiac arrhythmias, thromboses, pericardial and pleural effusion, appendicitis and perforated appendix, immune thrombocytopenia, chest pain, increased troponin levels, being in intensive care, and having anticoagulant therapy.
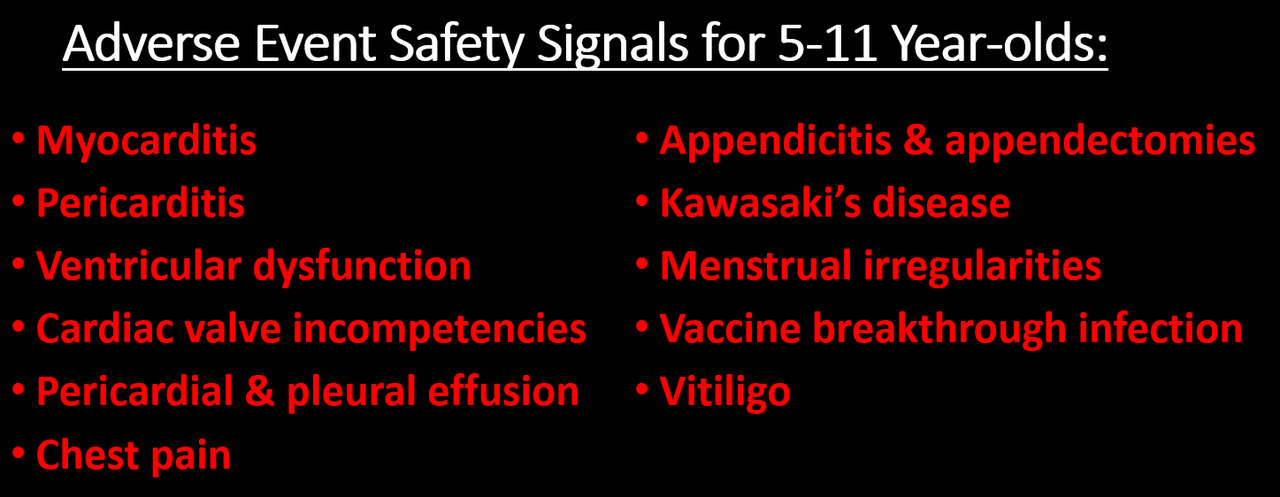
There are 66 safety signals for 5-11 year-olds, which include: myocarditis, pericarditis, ventricular dysfunction and cardiac valve incompetencies, pericardial and pleural effusion, chest pain, appendicitis & appendectomies, Kawasaki’s disease, menstrual irregularities, vitiligo, and vaccine breakthrough infection.
The safety signals cannot be dismissed as due to “stimulated,” exaggerated, fraudulent or otherwise artificially inflated reporting, nor can they be dismissed due to the huge number of COVID vaccines administered. There are several reasons why, but the simplest one is this: the safety signal analysis does not depend on the number of reports, but whether or not some AEs are reported at a higher rate for these vaccines than for other non-COVID vaccines. Other reasons are discussed in the full post below.
In August, 2022, the CDC told the Epoch Times that the results of their safety signal analysis “were generally consistent with EB [Empirical Bayesian] data mining [conducted by the FDA], revealing no additional unexpected safety signals.” So either the FDA’s data mining was consistent with the CDC’s method—meaning they “generally” found the same large number of highly alarming safety signals—or the signals they did find were expected. Or they were lying. We may never know because the FDA has refused to release their data mining results.
INTRODUCTION
Finally! Zachary Stieber at the Epoch Times managed to get the CDC to release the results of its VAERS safety signal monitoring for COVID-19 vaccines, and they paint a very alarming picture (see his reporting and the data files here, or if that is behind a paywall then here). The analyses cover VAERS reports for mRNA COVID vaccines from the period from the vaccine rollout on December 14, 2020 through to the end of July, 2022. The CDC admitted to only having started its safety signal analysis on March 25, 2022 (coincidentally 3 days after a lawyer at Children’s Health Defense wrote to them reminding them about our FOIA request for it).
[UPDATE: T Coddington left a link in comments to a website where he made the data in the Excel files more accessible.]
Like me, you might be wondering why the CDC waited over 15 months before doing its first safety signal analysis of VAERS, despite having said in a document posted to its website that it would begin in early 2021—especially since VAERS is touted as our early warning vaccine safety system. You might also wonder how they could insist all the while that the COVID-19 vaccines are being subjected to the most rigorous safety monitoring the world has ever known. I’ll come back to that later. First I’m going to give a little background information on the analysis they did (which you can skip if you’re up to speed) and then describe what they found.
BACKGROUND ON SAFETY SIGNAL ANALYSIS
Back in June 2022, the CDC replied to a Freedom of Information Act (FOIA) request for the safety signal monitoring of the Vaccine Adverse Events Reporting System (VAERS)—the one it had said it was going to do weekly beginning in early 2021. Their response was: we never did it. Then a little later they said they had been doing it from early on. But by August, 2022, they had finally gotten their story straight, saying that they actually did do it, but only from March 25, 2022 through end of July. You can get up to speed on that here.
The analysis they were supposed to do uses what’s called proportional reporting ratios (PRRs). This is a type of disproportionality analysis commonly used in pharmacovigilance (meaning the monitoring of adverse events after drugs/vaccines go to market). The basic idea of disproportionality analysis is to take a new drug and compare it to one or more existing drugs generally considered safe. We look for disproportionality in the number of adverse events (AEs) reported for a specific AE out of the total number of AEs reported (since we generally don’t know how many people take a given drug). We then compare to existing drugs considered safe to see if there is a higher proportion of particular adverse events reported for the new drug compared to existing ones. (In this case they are looking at vaccines, but they still use PRR even though they generally have a much better sense of how many vaccines were administered.)
There are many ways to do disproportionality analysis. The PRR is one of the oldest. Empirical Bayesian data mining, which was supposed to be done on VAERS by the FDA, is another. The PRR is calculated by taking the number of reports for a given adverse event divided by the total number of events reported for the new vaccine or the total number of reports. It then divides that by the same ratio for one or more existing drugs/vaccines considered safe. Here is a simple formula:
So for example, if half of all adverse events reported for COVID-19 vaccines and the comparator vaccine(s) are for myocarditis, then the PRR is 0.5/0.5 = 1. If one quarter of all AEs for the comparator vaccine are for myocarditis, then the PRR is 0.5/0.25 = 2.
Traditionally, for a PRR to count as a safety signal, the PRR has to be 2 or greater, have a Chi-square value of 4 or greater (meaning it is statistically significant) and there has to be at least 3 events reported for a given AE. (This also means that if there are tons of different AEs reported for COVID vaccines that have never been reported for any other vaccine, it will not count as a safety signal. I found over 6,000 of those in my safety signal analysis from 2021.
Ah yes, shared with the public — after first refusing to share the results and months of foot-dragging following repeated FOIA requests! We will see that the CDC has not done a more focused study on almost any of adverse events with “new patterns” (AKA safety signals).
SO WHAT DID THE CDC ACTUALLY DO?
The Epoch Times obtained 3 weeks of safety signal analyses from the CDC for VAERS data updated on July 15, 22 and 29, 2022. Here I will focus on the last one, since there is very little difference between them and it is more complete. The safety signal analysis compares adverse events1 reported to VAERS for mRNA COVID-19 vaccines from Dec. 14, 2020 through July 29, 2022 to reports for all non-COVID vaccines from Jan 1, 2009 through July 29, 2022.
PRRs are calculated separately for 5-11 year-olds, 12-15 year-olds and 18+ separately. For each age group, there are separate tables for AEs from all reports, AEs from reports marked serious and AEs from reports not marked as serious.2 Recall that a serious report is one that involves death, a life-threatening event, new or prolonged hospitalization, disability or permanent damage, or a congenital anomaly. I will focus on the reports for all AE’s.
They also have a table that calculates PRRs by comparing reports for the Pfizer COVID-19 vaccine to reports for the Moderna vaccine and vice versa, again for all reports, serious reports only and non-serious reports. There were no remarkable findings in those tables, so I will not discuss them. [Edit: I forgot what Norman Fenton noted in his analysis: the overall proportion of reports with serious adverse events is 9.6% for Modern compared to 12.6% for Pfizer.] This isn’t that surprising since both vaccines are very similar and so should present relatively similar adverse events when compared to each other, and any differences are likely not large enough to be picked up by a PRR analysis. [Though the difference in the overall rate of serious adverse events, which are not specific to a particular type of event only how serious it is, was significant.]
The CDC seems to have calculated PRRs for every different type of adverse event reported for all the COVID vaccines examined – though it’s possible they only analyzed a subset. What seems clear is that, among the AEs they examined, the only ones included in the tables satisfy at least one of two conditions: a PRR value of at least 2 and a Chi-square value of at least 4 (Chi is the Greek letter χ and is pronounced like ‘kai’). When both conditions were met, they highlighted the adverse event in yellow, which appears to indicate a safety signal. There were no COVID vaccine AEs listed with fewer than 3 reported events, though for non-COVID vaccines there were many AEs listed that had only 1 or 2 reported since 2009. The CDC tables still include these and highlight them in yellow when the PRR is greater than 2 and the Chi-square value is great than 4, indicating these events are counted as safety signals.
WHAT SAFETY SIGNALS DID THE CDC FIND?
I’m going to divide this up by age groups and the Pfizer v. Moderna comparison. Let’s start with the 18+ group.
There are 772 AEs that appear on the list. Of these, 770 are marked in yellow and have PRR and Chi-square values that qualify them as safety signals. Some of these are new COVID-19 related codes, and we would expect those to trigger a signal since they didn’t exist in prior years to be reported by other vaccines. So if we take those off, we are left with 758 different types of non-COVID adverse events that showed safety signals.
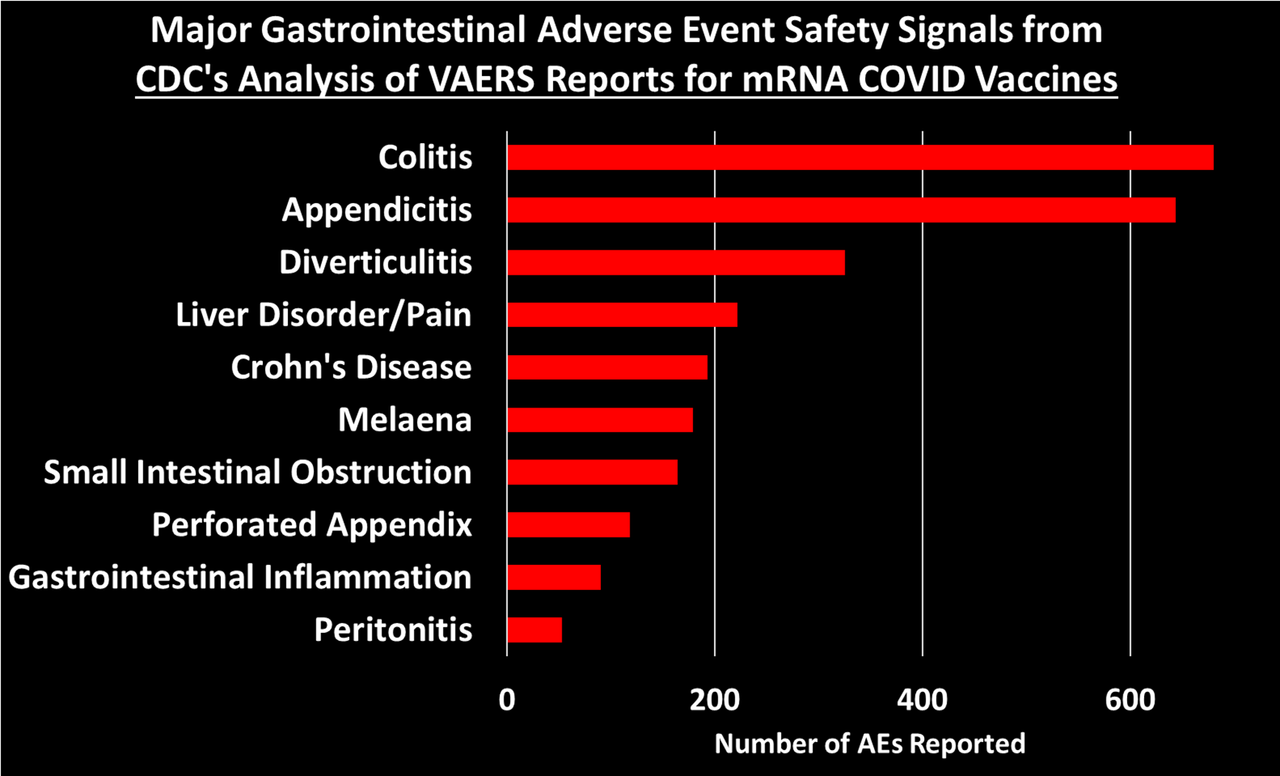
I grouped these 758 safety signals into different categories. The figure below shows the total number of AEs reported for each of the major categories of safety signals:
Let’s dig into some of these categories to look at what types of AEs generated the most number of reports:3
Let’s dig into some of these categories to look at what types of AEs generated the most number of reports:3
You can peruse the adverse events using the Excel tables provided by the CDC, which were posted by The Epoch Times and Children’s Health Defense at the links at the top of this post.
What about The Children?
If there is anything that looks remotely like a bright spot in all of this is that the list of safety signals for 12-17 and 5-11 year-olds is much shorter than for 18+. There are 96 AEs that qualify as a safety signal for the 12-17 group and 67 for the 5-11. When we take out the new COVID-era AEs, there are 92 safety signals for 12-17 year-olds and 65 for 5-11 year-olds. Here are the most alarming ones:
I don’t know why the list of AE’s is so much shorter for these age groups. It could be that the list of AE’s for other vaccines for these age groups is much shorter, so in a case where AEs have been reported for the mRNA COVID vaccines but not for other vaccines, it will not be counted as a safety signal by definition.
COMPARISONS TO MYOCARDITIS & PERICARDITIS
We are told that the existence of a safety signal doesn’t necessarily mean the AE is caused by the vaccine, and I accept that premise. But the current practice seems to be to ignore safety signals, dismiss them as noise without any evidence, and stall any investigation into them as long as possible. The precautionary principle, however, dictates we should presume that a safety signal indicates causality, until proven otherwise. Since, it has been acknowledged that the mRNA COVID vaccines can cause myocarditis and pericarditis (often referred to as myo-pericarditis), we can take those AEs as a kind of benchmark, and propose that, at minimum, any AE with a signal of equal or greater size should be considered potentially causal and investigated more thoroughly.4
After dropping the new COVID-era AEs, there are 503 AEs with PRRs larger than myocarditis (PRR=3.09) and 552 with PRRs larger than pericarditis (PRR=2.82).5This means that 66.4% of the AEs had a bigger safety signal than myocarditis and 77.3% were larger than pericarditis. You can see what those were by use this Excel file provided by the CDC and sorting the 18+ tab by the 12/14-07/29 PRR column (Column E). Then just look at which AEs have PRRs larger than the ones for pericarditis and myocarditis.
For 12-17 year-olds, there is 1 safety signal larger than myocarditis (it’s ‘troponin increased’) and 14 safety signals larger than pericarditis (excluding myocarditis), which include: mitral valve incompetence, bell’s palsy, heavy menstrual bleeding, genital ulceration, vaccine breakthrough infection, and a range of indicators of cardiac abnormalities.
For 5-11 year-olds, the comparison to myo/pericarditis is less germane, as they seem to suffer less from this side effect. But we can still make the comparison: there are 7 safety signals larger than pericarditis, including bell’s palsy, left ventricular dysfunction, mitral valve incompetence, and ‘drug ineffective’ (presumably meaning they still got COVID). There are 16 safety signals larger than myocarditis (excluding pericarditis), which in addition to those listed above also include: pericardial effusion, diastolic blood pressure increase, tricuspid valve incompetence, and vitiligo. Sinus tachycardia (high heart rate), appendicitis, and menstrual disorder come in just below myocarditis.
Now if we think of a safety signal as having both strength and clarity, then the PRR can be thought of as an indicator of how strong the signal is, while the Chi-square is a measure of how clear or unambiguous the signal is, because it gives us a sense of how likely the signal is due to chance alone: the larger the Chi-square value, the less likely the signal is due to chance. A Chi-square of 4 means there is only a 5% chance the observed signal is due to chance. A Chi-square of 8 means there is only a 0.5% chance of it being due to chance.6
For the 18+ group, there are 57 AEs with a Chi-square larger than myocarditis (Chi-square=303.8) and 68 with a Chi-square larger than pericarditis (Chi-square=229.5). Again, you can see what these are by going the Excel file linked above and sorting on Column D.
For the 12-17 group, there are 4 AEs with a larger Chi-square than myocarditis (Chi-square=681.5) and 6 larger than pericarditis (Chi-square=175.4).
For the 5-11 group, there are 22 AEs with a Chi-square larger than myocarditis (Chi-square=30.42) and 34 AEs with a Chi-square larger than pericarditis (Chi-square=18.86).
RESPONDING TO OBJECTIONS
Let’s dispense with some of the criticisms used to dismiss VAERS data, which will undoubtedly be raised if you try to bring the CDC’s analysis to people’s attention.
Objection: Anybody can report to VAERS. The reports are unreliable. Anti-vaxxers made lots of fraudulent reports. Nobody was aware of VAERS in the past, but now they are. So many people were afraid of the vaccine so they blamed all their health problems on it. Health workers were required by law to report certain adverse events, like deaths and anaphylaxis. Etc. Etc.
All of these objections ultimately rely on the notion that VAERS reports for COVID-19 vaccines have been artificially inflated over previous years for one reason or another. The thing of it is, though, that the CDC has a method for distinguishing between artificial inflation and real signal. The idea is simple: if adverse events are artificially inflated, they should be artificially inflated to the same degree. Meaning, the PRRs for all of these safety signals should be about the same. But even a casual glance at the PRRs in the Excel file show they vary widely, from as low at 2 to as high as 105 for vaccine breakthrough infection or 74 for cerebral thrombosis. This method does not on the number of reports, but the rate of reporting for certain events out of all events reported. If anything, this method would tend to hide safety signals in a situation where a new vaccine generates a very large number of reports.
The CDC has even done us the favor of calculating upper and lower confidence intervals, meaning that we can be at least 95% confident that two PRRs are truly different if their confidence intervals don’t overlap. So for example the lower confidence interval for pulmonary thrombosis is 19.7, which is higher than the upper confidence interval for 543 other signals. Artificially inflated reporting cannot explain why so many different adverse events have large PRRs that are statistically distinct from one another.
Objection: The safety signals are due to the huge number of COVID vaccines given out. Never before have we given out so many vaccine doses. By the end of July, the US had administered something like 600 million vaccine doses to people aged 18+. But the CDC analysis compares VAERS reports for these doses to all doses for all other vaccines for this age group since Jan. 1, 2009. But from 2015-2020 there were over 100 million flu doses administered annually to this age group alone. In previous work, I estimated 538 million doses of flu given to people 18+ from July 2015-June 2020. The number of flu and other non-COVID vaccines for this age group administered from Jan 1., 2009 through July 29, 2022 must be well over double this number, meaning VAERS reports for COVID vaccines are being compared to reports for at least double the number of doses for other vaccines. In addition to this, as already noted, the PRR methodology does not depend, strictly speaking, on the number of doses, but rather the rate of reporting of a specific AE out of all AEs for that vaccine.
Objection: the vaccines are mainly being given to older people who tend to have health problems, whereas other vaccines are given to younger people. This objection is dealt with, since the analyses are stratified by age groups. It might be still be somewhat valid for the 18+ group, except that in the safety signal analysis I did in the fall of 2021, I stratified by smaller age bands and still found safety signals. In any case, this objection is not enough to dismiss the safety signal analysis out of hand, but rather calls for better and more refined research.
Objection: The VAERS data is not verified and cannot be trusted. I’ll be the first person to agree that VAERS is not high quality data, but if it is completely untrustworthy, then how is it that the CDC uses these data to publish in the best medical journals such as JAMA and The Lancet? If the data were worthless, then these journals shouldn’t accept these papers. In that JAMA paper, they reported that 80% of the myocarditis reports met their definition of myocarditis and were included in the analysis. Many other reports simply needed more details for validation. Furthermore, the CDC has the ability and budget to follow-up on every report VAERS receives to get more details and even medical records to verify the report.
So if myocarditis shows a clear signal in the CDC’s analysis, and 80% of those reports were apparently high quality enough to be included in a paper published in one of the world’s top medical journals, how is it possible that all the rest of the reports are junk? That all of the other safety signals are meaningless? Answer: it isn’t.
And since we’re on the topic of safety signals that turned out to be real, it’s instructive to find appendicitis turn up as a safety signal in all 3 age groups, since a study published in NEJM based on medical records of over a million adult Israelis found an increased risk of appendicitis in the 42 days following Pfizer vaccination (but not following a positive SARS-CoV-2 PCR test). That study also found an increase in lymphadenopathy (swollen lymph nodes) after vaccination, but not after positive COVID test. Lymphadenopathy was another safety signal.
And that brings us to our last objection to be dispensed with: all of these AEs were due to COVID. There was an epidemic and so people were falling ill due to COVID and having all of these problems that were then blamed on the vaccine. Well to begin with, as we just saw, at least two of them (appendicitis and lymphadenopathy) do not appear to have increased risk ratios following a positive SARS-CoV-2 test, and we know that the mRNA vaccines increase risk of myo/pericarditis independent of infections. So how can we assume the rest of these are and dismiss them with the wave of a hand? We can’t. At minimum, they need further investigation. Furthermore, in the safety signal analysis I did in 2021, I dropped all VAERS reports where any sign of a SARS-CoV-2 exposure or infection was indicated on the report, and I still found large, significant safety signals.
PUTTING IT ALL INTO PERSPECTIVE
The Epoch Times article quotes my esteemed colleague and friend, Norman Fenton, Professor of Risk Management and an world renowned expert in Bayesian statistical analysis: “from a Bayesian perspective, the probability that the true rate of the AE of the COVID-19 vaccines is not higher than that of the non-COVID-19 vaccines is essentially zero…. The onus is on the regulators to come up with some other causal explanation for this difference if they wish to claim that the probability a COVID vaccine AE results in death is not significantly higher than that of other vaccines.” (See his post on the CDC analysis here.) The same is true for all the safety signals they found.
The CDC’s VAERS SOP analysis document lists 18 Adverse Events of Special Interest says they are going to pay close attention to. In their 2021 JAMA paper (and similar presentations to ACIP), the researchers responsible for analyzing the millions of medical records in the CDC’s Vaccine Safety Datalink (VSD) using the ‘Rapid Cycle Analysis’ only studied 23 outcomes. A Similar analysis in NEJM from Israeli researchers focused on only 25 outcomes. Compare this to over 700 safety signals found by the CDC when they finally decided to look—and that’s not even counting all the adverse events that have never been reported for other vaccines so cannot ever show a safety signal by definition. How can the CDC say that these safety signals are meaningless if almost none of them have been studied any further? And yet we are assured that these vaccines have undergone the most intensive safety monitoring effort in history. It’s complete and utter hogwash!
* * *
Josh Guetzkow is a senior lecturer at The Hebrew University of Jerusalem. Subscribe to his Substack here.
1) To be precise, the ‘adverse events’ are for ‘preferred terms’ (PTs) which is a type/level of classification used in the Medical Dictionary for Regulatory Activities (MedDRA), which is the classification system used by VAERS and in other pharmacovigilance systems and clinical research for coding reported adverse events. Not all preferred terms are a symptom or adverse event per se. Some refer to a specific diagnostic test that was done or a treatment that was given.
2) It’s not entirely clear how they divided these up, since there are clearly AEs that should be considered serious that don’t show up in the serious Excel table — though maybe they don’t come up simply because they are looking within serious reports. I believe that they just filtered the reports to include only serious reports or non-serious reports, then did the safety signal analysis on all the AE’s coded in those reports. The reason I think this is that I used the MedAlerts Wayback Machine, selected just the serious COVID-19 vaccine reports, and the numbers of total reports was very close to the one in the table provided by the CDC (MedAlerts actually had a bit less). The files obtained by the Epoch Times do not include much in the way of a description as to how the analyses were done, so I had to infer some details, which might be incorrect. I will try to note when I am drawing an inference about how the analysis was done.
3) Generally speaking, these figures show the top ten AEs in each category. In some cases I combined AEs that indicated the same thing, such as combining ‘heart rate irregular’ with ‘arrythmia.’ [UPDATE: Note that the charts of all categories, cardiac and thrombo-embolic events were updated on Jan 7, 2023. The reason is that I had previously categorized acute myocardial infarction as a cardiac issue and myocardial infarction as thrombo-embolic. To be consistent, I have now combined myocardial infarction and acute myocardial infarction into one AE category in the thrombo-embolic events (which made the total AEs reported for that category larger than for pulmonary ones) and then added a different cardiac AE to the cardiovascular AE category, ventricular extrasystoles, AKA premature ventricular contraction (PVC), which dependent on frequency and the presence of other cardiomyopathies is associated with sudden cardiac arrest.]
4) Note that using the myo-pericarditis signal as a yardstick doesn’t mean that these are the only signals that matter. To give one example, anaphylactic reactions don’t even show up in the list of safety signals, even though that was one of the very first risk of the vaccine that became apparent from day one of the vaccine rollout.
One potential objection to this benchmark is that it is too low of a bar, since myo-pericarditis appears to disproportionately affect younger men and so a proper safety signal should be stratified by age and gender then compared with myocarditis similarly stratified. I agree, and it is the CDC’s job to do that. But the fact is that any adverse reaction might disproportionately affect some subgroup of people, in which case the safety signal for that group would be similarly faint or diluted when we look at everyone together. So objection overruled.
5) In their Standard Operation Procedures document, the CDC said they would combine these and related codes together to assess a safety signal, but never mind – at least they finally got around to doing something.
6) In this context, the Chi-square is largely driven by the sheer number of adverse events: the more adverse events reported, including for the comparator vaccine, the larger the Chi-square. For example, the PRR for pericarditis and subdural haematoma is the same (2.82), but there were 1,701 incidents of pericarditis reported for mRNA COVID vaccines versus 221for the comparator vaccines, with Chi-square of 229.5. For subdural haematoma, these numbers are 162 verus 21, for a Chi-square of 21.2.
Mounting evidence shows the COVID shots are destroying people’s immune systems and are triggering turbo-charged cancers
A survey by Steve Kirsch found sudden death is the No. 1 cause of death among those under the age of 65 who got the COVID jab
Myocarditis as a cause of death is now registering across all age ranges but only for the vaccinated. Cardiac-related deaths are also significantly elevated among younger people (under 65) who got the jab compared to their unjabbed peers
Recent research shows repeated jabs trigger a switch in the types of antibodies your body produces and lower your ability to clear viruses. By switching from spike-specific neutralizing IgG antibodies to IgG4 antibodies, your body switches from tumor suppression mode into tumor progression mode
In addition to the potential for cancer cells to run amok, IgG4 dominance may also have severe autoimmune implications, as the COVID jab spike protein share similarities with human proteins
Evidence showing the COVID shots are a public health disaster keeps mounting. In late December 2022, Steve Kirsch1 and Jessica Rose,2 Ph.D., both published Substack articles detailing some of the latest evidence showing the shots are destroying people’s immune systems and have triggered an avalanche of turbo-charged cancers.
Kirsch’s article3 features results from a recent survey he conducted. It included four questions: age, whether the deceased was jabbed or not, year of death and cause of death. While the number of responses is low, major insights can still be gleaned by looking at the trends.
First, we have the baseline data from 2020, which show cancer was the No. 1 killer of Americans younger than 65, followed by hospital treatment for COVID. Turbo-charged cancers accounted for one-ninth of the cancer reports, and there were no reports of death from myocarditis.
Among seniors over the age of 65, preexisting conditions were the top cause of death in 2020. Cancer was second, COVID infection third and cardiac events fourth. There were no turbo-charged cancer deaths, nor any myocarditis deaths. Kirsch then gets into the differences between the vaxxed and the unvaxxed in 2021 and 2022.
What the Unvaxxed Died of in 2021 and 2022
In 2021 and 2022, the primary cause of death for people 65 and younger was hospital treatment for COVID. Incidences of sudden death, pulmonary embolism and turbo-charged cancers were all low, and there were no unknown causes of death, nor any myocarditis deaths.
The same went for people older than 65. Hospital treatment for COVID was the No. 1 killer. Heart attacks, turbo-charged cancer and sudden death were all low, and there were no deaths from myocarditis.
What the COVID-Jabbed Died of in 2021 and 2022
Among the COVID-jabbed aged 65 and younger, sudden death was the No. 1 cause of death in 2021 and 2022. The second was cardiac-related death and cancer was third. Importantly, the incidence of turbo-charged cancer among the jabbed was significant in this group, and myocarditis killed more than COVID-19.
Among those older than 65, cancer was the No. 1 cause of death, and the turbo-charged cancer rate is “huge compared to those without the vaccine.” Sudden death was also significantly elevated.
Stark Difference in Cancer Deaths Between Jabbed and Unjabbed
Kirsch summarizes the three most stunning differences between the jabbed and unjabbed:4
1.“Sudden death rates are off the charts for the vaccinated cf. unvaccinated for those <65 … It’s the #1 cause of death for this age group …
2.Myocarditis as a cause of death is registering now for both age ranges but only for the vaccinated …
3.Cardiac issues as a cause of death in vaccinated young people (<65) are significantly elevated vs. their unvaxxed peers.”
How COVID Jabs Raise Risk of Infections and Cancer
Exploding cancer rates is precisely what you would expect from a drug that impairs and destroys your immune system, which is what the COVID jabs do. The scientific paper “Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations”5 describes how the COVID shots suppress your innate immune system by inhibiting the type-1 interferon pathway, which is the first-stage response to all viral infections.
The reason type-1 interferon is suppressed is because it responds to viral RNA, and there’s no viral RNA in the COVID shot. The RNA is modified to look like human RNA, so the interferon pathway doesn’t get triggered. As a result, the COVID jab makes you more susceptible to infections.
One mechanism by which the jab causes cancer has to do with the fact that the SARS-CoV-2 spike protein obliterates 90% of the DNA repair mechanism in lymphocytes,6 a type of white blood cell that helps your body fight infections and chronic diseases such as cancer. That’s bad enough, yet that’s just one mechanism of many.
How the Jab Lowers Your Viral Clearance Capacity
Recent research7,8 also shows that repeated jabs trigger a switch in the types of antibodies your body produces and lower your ability to clear viruses. Jessica Rose reviews these findings in her Substack article:9
“A paper was published in Science Immunology on December 22, 2022 entitled: ‘Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination’10 …
[It] explains in wonderful detail how a class of antibody that commands a non-inflammatory response (more like tolerizing) is prominent in people who have been repeatedly injected with the modified mRNA COVID-19 injectable products.
Translation: Instead of the intended pool of spike-specific neutralizing IgG antibodies being dominant in multiply-injected people, a pool of antibodies associated with spike-specific tolerance are dominant in multiply-injected people.
Besides the tolerizing capacity, they also showed that the phagocytic enabling capacities were much reduced overall. These activities lead to clearance of viral pathogens. Reduce them → reduction in viral clearance capacity …
To be clear, this wasn’t a ‘maybe the antibody profile was a little different’ … This was a ‘whoa there’s a 48,075% increase in spike-specific antibodies between the 2nd and 3rd injections …
IgG4 antibodies among all spike-specific IgG antibodies rose on average from 0.04% shortly after the second vaccination to 19.27% after the third … [I]mportantly, that is not a typical consequence of repeat antigen exposure from either natural infections and vaccination.”
Spike Overexposure Also Opens the Door for Cancer
As noted by Substack author Brian Mowrey:11
“This is a totally bonkers thing for an anti-spike-protein B cell to decide to do, and reflects B cell over-exposure to spike, which reflects super-excess production of spike by the Pfizer/BioNTech mRNA code …
It is not normal to make IgG4 when repeat encounter with a virus is spaced out over a lifetime, but injection-prompted antigen exposure promotes this response, and mRNA vaccines accelerate this effect …
There is no reason to predict that this would be ‘good’ in an antiviral response … ‘Wearing out’ the immune response in this way is believed to contribute to the development of tolerance against tumors.”
So, to summarize the effects in layman’s terms, the switch from spike-specific neutralizing IgG antibodies to IgG4 antibodies switches your body from tumor suppression mode into tumor progression mode, as cancerous cells now can evade your immune system. You become “tumor tolerant” as your immune system is no longer scavenging for and eliminating cancer cells. Mowrey also points out that:12
“Once a B cell has switched to IgG4, it cannot switch to any other IgG subclass, as the genes for all those other base designs have been discarded. All future clones of this B cell will code for IgG4 receptor/antibody for the antigen in question.”
What Other Health Effects May Result?
For clarification, IgG4 is a subclass of the immunoglobulin G (IgG) antibody type that responds to repeated and/or long-term exposure to an antigen. The mRNA shot evaluated here was that of Pfizer, and it was compared against Janssen’s viral vector-based shot. Moderna’s shot was not included. Notably, these results were not found among people who got Janssen’s shot, only Pfizer’s Comirnaty jab.
As noted by Rose:13
“… the bottom line here is that the Comirnaty product … induces a shift away from a viral clearing to a tolerance-inducing antibody class, and this is not the status quo for traditional vaccines or natural infections. The main problem here is … we have no idea of the effects of this ‘effect.'”
That said, we can look at what happens in people with IgG4-related disease, and start formulating hypotheses from there. As explained by Rose, a hallmark of IgG4-related disease is fibrosis, i.e., tissue scarring, which can lead to organ dysfunction, organ failure and even death if left untreated.
Rose is now researching the possible links between this antibody switching and the stringy white deposits found in COVID-jabbed people who died. Might it be a new form of connective tissue disease?
In addition to the potential for cancer cells to run amok (as discussed in the section above), IgG4 dominance may also have severe autoimmune implications seeing how the COVID jab spike protein share similarities with human proteins.
“Molecular mimicry has been shown14 in multiple publications to be a potential problem with regard to the spike protein whereby it has been shown to share motifs with human proteins,” Rose writes.15“What this means is that autoimmunity potential against these human proteins is clear and present.
In the context of this recent publication showing a dominant IgG4 pool, I have to wonder what the implications of this dominant pool are for molecular mimicry. Are these IgG4 antibodies capable of tolerizing in the context of our own protein?”
Resources for Those Injured by the COVID Jab
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system.
The same goes for anyone who has taken one or more COVID jabs and had the good fortune of not experiencing debilitating side effects. Your health may still be impacted long-term, so don’t take any more shots.
When it comes to treatment, there are still more questions than answers, and most doctors are clueless about what to do — in part because they never bothered to give early treatment for COVID and therefore don’t understand how different medicines and supplements impact the spike protein.
So far, it seems like many of the treatments that worked against severe COVID-19 infection also help ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
Both agree that eliminating the spike protein your body is now continuously producing is a primary task. Perro’s preferred remedy for this is hydroxychloroquine, while Kory’s is ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein.
As a member of the Front Line COVID-19 Critical Care Alliance (FLCCC), Kory helped develop the FLCCC’s post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com16 (hyperlink to the correct page provided above).
The World Health Council has also published lists of remedies that can help inhibit, neutralize and eliminate spike protein. Inhibitors that prevent spike protein from binding to your cells include Prunella vulgaris, pine needle tea, emodin, neem, dandelion extract and the drug ivermectin.
Spike protein neutralizers, which prevent the spike from damaging cells, include N-acetylcysteine (NAC), glutathione, fennel tea, star anise tea, pine needle tea, St. John’s wort, comfrey tea and vitamin C. A March 2022 review paper17 suggests combating the neurotoxic effects of the spike protein using the flavonoids luteolin and quercetin.
•Lower your Omega-6 intake. Linoleic acid is consumed in amounts ten times of ideal in well over 95% of the population and contributes to massive oxidative stress that impairs your immune response. Seed oils and processed foods need to be diligently avoided. You can review my previous post for more information.
•Pharmaceutical grade methylene blue, which improves mitochondrial respiration and aid in mitochondrial repair. It’s actually the parent molecule for hydroxychloroquine. A dose of 15 to 80 milligrams a day could go a long way toward resolving some of the fatigue many suffer post-jab.
It may also be helpful in acute strokes. The primary contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all. To learn more, see “The Surprising Health Benefits of Methylene Blue.”
•Near-infrared light, as it triggers production of melatonin in your mitochondria18 where you need it most. By mopping up reactive oxygen species, it too helps improve mitochondrial function and repair. Natural sunlight is 54.3% infrared radiation,19 so this treatment is available for free. For more information, see “What You Need to Know About Melatonin.”
•Lumbrokinase and serrapeptidase are both fibrinolytic enzymes taken on an empty stomach one hour before or two hours after to help reduce the risk of blood clots.
Three military doctors have blown the whistle on the devastating effects of forced COVID-19 vaccinations on American troops.
According to the whistleblowers, medical billing code data captured by the Defense Medical Epidemiology Database (DMED), which is run by the Department of Defense (DoD), shows that rates of miscarriage, myocarditis, cancer, Bell’s palsy, female infertility, and many more serious health conditions have risen dramatically since vaccines were made mandatory.
Naturalnews.com reports: Cancer rates are particularly concerning, they say, as the normal average number of new cases per year is about 38,700, based on the time period from 2016-2020. In 2021 after Operation Warp Speed was launched, however, the number of new cancer cases that year rose to 114,645.
The Armed Forces Health Surveillance Branch (AFHSB) runs the DMED, which it describes as a “web-based tool to remotely query de-identified active component personnel and medical event data contained within the Defense Medical Surveillance System (DMSS).”
“The database contains every International Classification of Diseases (ICD) medical billing code for all medical diagnoses submitted by the military for medical insurance billing,” reports explain. (Related: Remember at the launch of Operation Warp Speed when Dr. Sara Beltrán Ponce, MD, suffered a horrific miscarriage right after getting jabbed for the Chinese Flu?)
Neurological issues up 1,000% in military following Operation Warp Speed
The three military whistleblowers in question are Samuel Sigoloff, Peter Chambers, and Theresa Long. Attorney Thomas Renz issued sworn statements from these three to the courts as part of a major lawsuit.
During the first 10 months of 2021, Renz says, miscarriages alone rose by 300 percent in the military. His hope is that the suit will lead to an end for covid jab mandates in the military.
Sen. Ron Johnson (R-Wisc.) is also involved, having recently hosted “COVID-19: A Second Opinion,” a livestreamed discussion panel featuring numerous world-renowned doctors and medical experts who offered a much different take on the scamdemic and how the government handled it.
On February 1 of this year, Johnson wrote a letter to U.S. Secretary of Defense Lloyd Austin. In it were the findings from a roundtable on covid jab injuries and deaths, including data showing a 10-fold increase in neurological issues post-Operation Warp Speed.
Johnson also revealed the following increases in other health conditions following the mandate of covid injections in the military:
Hypertension: 2,181 percent increase
Nervous system disorders: 1,048 percent increase
Malignant neoplasms of esophagus: 894 percent increase
Multiple sclerosis: 680 percent increase
Malignant neoplasms of digestive organs: 624 percent increase
Guillain-Barre syndrome: 551 percent increase
Breast cancer: 487 percent increase
Demyelinating: 487 percent increase
Malignant neoplasms of thyroid and other endocrine glands: 474 percent increase
Female infertility: 472 percent increase
Pulmonary embolism: 468 percent increase
Migraines: 452 percent increase
Ovarian dysfunction: 437 percent increase
Testicular cancer: 369 percent increase
Tachycardia: 302 percent increase
Between the years of 2016 and 2020, there were 1,499 codes for miscarriage reported each year. From January through October 2021 – not even a full year – there were an astounding 4,182 miscarriages logged into the system.
During his panel, Johnson further made note that it appears myocarditis rates are being doctored by the government. Back in August 2021, it was shown in the codes that myocarditis diagnoses were up 2,800 percent. This month, however, it is now listed as only 200 percent higher.
“There appears to be doctoring of the data,” Johnson stated. “Now, my staff has already sent – this morning, we sent a record preservation letter to the Department of Defense to try and protect this data.”
“Our soldiers are being experimented on, injured, and sometimes, possibly, killed,” he added in a statement.