Leading experts in Japan have just put out an emergency global warning as the nation is about to roll out dangerous new “self-amplifying” Covid mRNA “vaccines” for public use.
A group of scientists and a top Japanese lawmaker have just held a press conference to raise the alarm over the new “vaccines,” warning they will “trigger a worldwide disaster.”
The controversial new “self-amplifying” Covid mRNA “vaccine” was developed by an obscure San Diego-based biotech company called Arcturus Therapeutics Holdings Inc.
Arcturus Therapeutics, which is also an emerging pharmaceutical company, recently had its self-amplifying mRNA vaccine become accepted by Japanese regulators.
Japan’s Ministry of Health, Labor, and Welfare (MHLW) granted approval for ARCT-154, a self-amplifying mRNA (sa-mRNA) COVID-19 vaccine.
The shot will be used for initial vaccination and booster for adults 18 years and older.
This new Covid sa-mRNA vaccine targeting was developed by Arcturus Therapeutics in partnership with Melbourne, Australia-based CSL.
In October the Japanese health authorities will roll the sa-mRNA Covid vaccine out to the population.
The approval is based on positive clinical data from several ARCT-154 studies, including an ongoing 16,000-subject efficacy study performed in Vietnam.
Initial study results have been published in MedRxiv and are expected to be published in a peer-reviewed journal by the end of the year.
However, the approval of the experimental vaccines has been met with a widespread backlash from Japanese scientists and medical experts, who have already been sounding the alarm about the “traditional” mRNA injections.
In response to the looming rollout of the new shots, Japanese Member of Parliament Ryuhei Kawada led an emergency press conference in Japan to warn the public.
At his event, he and colleagues expressed great concern about the country’s upcoming launch of the “mRNA replicon vaccines.”
During the press conference, Kawada argued that the October 1 deployment effort involving the COVID-19 vaccines “should be halted.”
Citing a study published in Cell, scientists looked at how something similar to the replicon mRNA vaccine worked when put into cells.
They found that the vaccine parts kept increasing inside the cells.
Experts are warning that these self-replicating mRNA vaccines continue to replicate in an out-of-control manner throughout the cells and more of the body.
The concern would be that particulas known as extracellular vesicles (including exosomes) could lead to shedding via bodily fluids and the like.
The Japanese regulators and Arcturus Therapeutics are refusing to discuss such risks, however.
“We are addressing this press conference from the standpoint that the replicon vaccine should be halted,” Kawada said during the presser.
“Therefore, we have decided to hold this emergency press conference.
“This self-replicating immune agent, scheduled to start regular vaccinations from October 1st, ought to be halted, and I strongly advocate for this action.
“Additionally, we must ensure thorough investigation and verification to provide relief to mRNA vaccine victims who have suffered significant harm.
“This must be systematically carried out.
“Instead of merely discarding unused vaccines, we should facilitate research by passing them on to researchers for analysis.
“I intend to make these demands to the Prime Minister and the Ministry of Health, Labour and Welfare.”
Professor Dr. Seiji Kojima of Nagoya University also raised concerns about the new injections.
“Compared to those who are unvaccinated, the mortality rate is five times higher if you get vaccinated twice,” Prof. Kojima warned.
“The purpose of receiving vaccination is indeed to reduce the mortality rate, but ironically, the rate was five times higher after receiving the vaccine.”
Professor Murakami of Tokyo Science University also expressed similar concerns.
“Japan is planning a large-scale rollout of self-amplifying vaccines, which are considered hazardous materials…” Murakami told the Japanese people.
“…by the beginning of next month, Japan has the potential to trigger a worldwide disaster.”
“The vaccines do not seem to be effective,” he warned.
“They do not work. They lack efficacy.
“mRNA vaccines have resulted in many deaths, injuries, and victims.”
“Despite knowing they are ineffective, their use could possibly cause significant international damage,” Prof. Murakami added.
“There is also the possibility of person-to-person transmission.
“There is absolutely no need to administer it. There is no need at all.
“Therefore, knowing this and still administering the vaccine, I believe, is a crime. ”
WATCH:
VIDEO LINK: https://rumble.com/v5fsecl-japan-warns-self-amplifying-mrna-vaccines-will-trigger-worldwide-disaster.html
Do you remember back during the Planscamdemic when Dr. Charles Lieber of Harvard University’s chemistry department was arrested for not disclosing financial relationships with…(cough)… laboratories in China? Do you also remember when it was revealed that his “specialty” was revealed to be how to use nano-particles and how they might in turn be used to carry drugs into the brain past the blood-brain barrier? And do you remember who that touched off an internet scramble to investigate all the implications of nano-particles and covid mRNA injections, and how people quickly found patents by Baal Gates who wanted to create an “updatable” quackcine technology that you wore in your body, and updated like those never-welcome-take-forever Windows updates? Remember how some people speculated that to make such a technology work, it would have to be via nano-particles being implanted somehow in the body (hmmm…. I wonder how?), particles which in turn would respond to certain types of electromagnetic signals contituting the “update” from the quackcine company? (For convenience’s sake, let’s call that company Microcrud-Nanoshinola LLC). Do you remember when some started drawing connections between all of this and the quackcines and the adverse reactions? Remember how The Science and The Media said that making connections between all of this – the planscamdemic, the arrest of Lieber, the patents and quackcine schemes of Baal Gates – were all kooky conspiracy theorists/
Well… two doctors in Korea are confirming at least part of this scenario according to the following article shared by V.T. (with our thanks):
Confirming what many suspected to be the case, two Korean scientists have found that the mRNA vaccine vials from both Pfizer-BioNTech and Moderna contain self-assembling nanoparticles that form into the white clots that many embalmers are discovering inside the bodies of the “fully vaccinated.”
The findings of these two scientists closely resemble what Mike Adams, the Health Ranger, found when he reported on these embalmer clots back in January 2022. (Be sure to check out this report highlighting the footlong clots found in some fully vaccinated dead bodies.)
What Adams apparently found concerning these clots is that they are not composed of actual human tissue, nor do they contain amyloid proteins, according to Dr. Ruby – so what are they, exactly?
If that’s the case, then what of the mechanism for the update from Microcrud-Nanoshinola LLC? What is interesting to me is that this article actually goes there; what was “conspiracy theory” a few short years ago is now a possibility that is being considered:
The clots in question apparently contain magnetic graphene that grows in both arteries and veins. In some cases, the resulting clot is upwards of three feet in length and could be used as an antenna system for WiFi signals to connect the fully jabbed to “the borg.”
“Can you hear a high pitch frequency that increases in amplitude at night?” the X account that reiterated all of this asked of Dr. Ruby, who confirmed that she is aware of this having “broke the worldwide story of La Quinta Columna and the graphene oxide as well as the first embalmer report.”
The real question left unanswered by the article’s high octane speculation is why would one want to inject such nano-particles into someone for the purposes of Wifi signal reception, when the injection only causes the people receiving them to die? What use is a dead antenna? Is it, as the appended video in the article suggests, to somehow create “zombies”, a “fake general resurrection” by creating massive nervous reactions in dead people via strong electromagnetic pulse? (It sounds crazy, I know, but then again, these people are bat-shinola crazy.) Perhaps, perhaps not. What is intriguing here is the apparent discovery of graphene and other metals in some of the injections, which can act as antenna.
I find all this intriguing because I have a friend with Morgellon’s disease, remember that one? This was a strange disease that some people began to report during the 1990s and early 2000s. We were assured by The Science and The Media that there was no such disease and that it was just all some sort of mass hypercondria. But what many of these people reported was a sensation of tingling, like ants crawling under their skin. They reported lesions, and these in turn would be focuses for the feeling that insects were crawling under their skin. Some reported being particularly sensitive to increased electromagnetic background noise. Then in my friend’s and a few other people’s cases, a physician, Dr. Hildegard Stavanger, stepped forward to actually investigate – that’s called science, folks, as distinct from The Science – and what she discovered was nothing less than amazing: tiny “plastic” nano-fibers, many of them growing in the lesions of her patients. These in turn acted like tiny nano-antennae, and when electromagnetic background radiation increased, sure enough, the Morgellon’s victims’ pain increased. Many, as a result of these early findings, speculated that the nano-fibers were entering the bodies of the victims through the so-called “chemtrail” spraying that many alleged was going on. Others looked to genetically modified foods. The latter may seem an even more unlikely candidate, but it should be remembered that in the wake of quackcine skepticism during the planscamdemic, it was alleged that members of the Technokookracy including Baal Gates advocated putting the quackcines into the GMOs, and with that, the nano-particles, GMO foods, and whatever sick and twisted agenda was behind all of this, linked up again. The story about Gates, so we’re told, was false:
What’s interesting, however, is that the basic conceptual point is not denied by the “fact check” in that vaccine-via-food is an admitted research goal:
Uh huh. Just like no program of nano-particles was being studied here by Dr. Lieber, either. And as for genes crossing into other species, check this out:
My point here is that all of this high octane dot-connecting is not implausible.
All of this brings us to the real question squatting like a big fat ugly toad in the middle of all this swirling cloud of disconnected dots: who is poisoning us, and why? It seems evident to anyone with a real brain who is not leaping onto the propaganda bandwagon of The Science and The Media, that someone very much wants us dead; our food supply is poison, our drugs are poison, our “vaccines” have been redefined so that hugely experimental injections can be called vaccines and tested on human populations under the guise of a “health emergency”, and many people taking those “safe and effective” injections are suffering, or have died, in cruel fashions. And The Media and The Science are silent (and The Science is enjoying a well-paid retirement, apparently). So… again… who wants us dead so badly, and why? I have a few ideas, but I’d like to hear yours.
But whatever we make of it, some doctors in some countries haven’t entirely lost their minds, and are willing to say what needs to be said. Shame on all the big networks of the American propataintment media for not even bothering with the story.
See you on the flip side…
(If you enjoyed today’s blog, please share it with your friends.)
THIS IS JUST A VERY GREATLY ABBREVIATED LIST OF VACCINE INJURIES COMPILED BY K.C. SHE HAS LISTS AND LISTS OF ARTICLES AND STUDIES TO BACKUP HER WORK.
GO TO THE LINK TO PERUSE THEM ALL: https://ladycasey.substack.com/p/scientific-studies-on-vaccine-injuries?utm_source=substack&utm_campaign=post_embed&utm_medium=email
This post mainly consists of scientific studies (both peer reviewed and preprints), systematic reviews, case studies (a few key ones of the thousands out there), and other medical journal articles that support the assertions in my Vaccine Injury post from November 2022. I began bookmarking these studies in late 2021, but since I’ve surely missed some, this is not a comprehensive list. It is, however, significant enough to utterly debunk the “safe and effective” propaganda of the past three years. (I will continue adding to this list indefinitely, so please check back on occasion for the most recent scientific discoveries about C19 vaccine injuries.)
I’m not a scientific researcher, data analyst, or medical professional. Neither are most of my readers. However I, and presumably they/you, are fully intellectually capable of reading and understanding the discussions and conclusions in most of the studies listed below. For those of you who prefer to skim, in most cases, after each link below, I include a short (2-3 sentence) summary of the study’s conclusions.
Some of the studies below are followed by a supporting article explaining its findings in layman’s terms. All such articles are written by experts in their field, including scientific researchers, professors, data analysts, PhDs, MDs and other medical professionals. (Some accompanying articles are under a paywall, for which I apologize, however I’m happy to email my readers free versions of any linked articles upon request.)
Lastly, please take note that much of the pro-jab jargon used in these studies is required to survive peer review. Journals are beholden to (funded and captured by) the pharmaceutical industry. Researchers have stated outright that they cannot get published on this topic without the inclusion of pro-vaccine rhetoric in their studies.
Please use this post as a resource to backup your own arguments with uninformed acquaintances who continue to believe and perpetuate the false government/Pharma narrative that the C19 “vaccines” are safe. They are not, and the following evidence couldn’t be more clear about that.
General Adverse Events
Serious Adverse Events of Special Interest Following mRNA Vaccination in Randomized Trials https://www.sciencedirect.com/science/article/pii/S0264410X22010283
(Peter Doshi—senior editor of the BMJ—study concluding that Covid vaccines were associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated. And that the excess risk of serious adverse events of special interest surpassed the risk reduction for COVID-19 hospitalization. Explanatory articles here, here, and here.)
COVID-19 Modified mRNA “Vaccines” Part 1: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex https://www.ijvtpr.com/index.php/IJVTPR/article/view/101
(“The usual safety testing protocols and toxicology requirements were bypassed. Many key trial findings were either misreported or omitted entirely from published trial reports. By implication, the secondary estimates of excess morbidity and mortality in both trials must be deemed underestimates. Rigorous re-analyses of trial data and post-marketing surveillance studies indicate a substantial degree of modmRNA-related harms than was initially reported. Confidential Pfizer documents had revealed 1.6 million adverse events by August 2022. A third were serious injuries to cardiovascular, neurological, thrombotic, immunological, and reproductive systems, along with an alarming increase in cancers. Moreover, well-designed studies have shown that repeated modmRNA injections cause immune dysfunction, thereby potentially contributing to heightened susceptibility to SARS-CoV-2 infections and increased risks of COVID-19. This paper also discusses the insidious influence of the Bio-Pharmaceutical Complex, a closely coordinated collaboration between public health organizations, pharmaceutical companies, and regulatory agencies.” Read the original paper here and explanation of its highly suspect & unethical redaction here.)
Potential health risks of mRNA-based vaccine therapy: A hypothesis https://www.sciencedirect.com/science/article/pii/S0306987723000117
(“If our hypothesis were to be confirmed, the implications for public health would be staggering and appalling in the context of the mass-scale COVID-19 vaccination already taking place, particularly if the nms-mRNA enters brain, bone marrow, and – if already present in the vaccinee – cancerous or pre-cancerous cells, or if the vaccine is administered to females early in their pregnancy and the nms-mRNA transfects embryonic cells.”)
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA https://www.mdpi.com/2227-9059/11/8/2287
(“This paper reviews autoimmune, cardiovascular, neurological, potential oncological effects, and autopsy evidence for spikeopathy.” Also, ” Treatment modalities for ‘spikeopathy’-related pathology in many organ systems, require urgent research and provision to millions of sufferers of long-term COVID-19 vaccine injuries. We also advocate for the suspension of gene-based COVID-19 vaccines and lipid-nanoparticle carrier matrices, and other vaccines based on mRNA or viral-vector DNA technology.” Comprehensive explanatory article here.)
The Novelty of mRNA Viral Vaccines and Potential Harms: A Scoping Review https://www.mdpi.com/2571-8800/6/2/17
(The COVID-19 vaccines are known to be unsafe for several reasons: 1) the Wuhan Spike protein damages cells, tissues, organs, and causes blood clotting, 2) the lipid nanoparticles may have toxicity from the PEG or polysorbate 80 or from syncytia formation, 3) the mRNA appears to be resistant to ribonucleases and is not broken down in the body. As some point the mRNA or fragments could interfere with gene function or alter other microRNAs that are managing the human genome. Explanatory article here.)
The COVID shots are known to increase in lethality after repeated doses. The ‘vaccines’ are linked to turbocancers, reproductive destruction, miscarriages in pregnant women, paralyzation, tinnitus, increased excess death rates, autoimmune disorders in the thyroid, headaches, seizures, heart inflammation and more. Children who received mRNA ‘vaccines’ have also been affected. The mRNA jabs contain hundreds of times the allowable levels of DNA contamination leading to mutagenic effects that change genetic material and increase mutations, contaminating the blood supply, and permanently altering the DNA of the vaccinated and their offspring. Dr. Peter McCullough estimated that over 600,000 Americans have died from COVID ‘vaccines’. The jabs are expected to kill people for a very long time into the future.
The McCullough Foundation published a new study that proposes an intervention to turn off the mutagenic effects of COVID mRNA injections by using small interfering RNA (siRNA) to bind to COVID vaccine mRNA so that the body may eliminate it, and ribonuclease targeting chimeras (RIBOTAC) that can sandwich the mRNA. The introduction of siRNA and RIBOTAC may potentially prevent uncontrolled Spike protein production and reduce toxicity. The targeted nature of siRNA and RIBOTACs allows for precise intervention to inactivate and degrade residual vaccine mRNA, offering a path to prevent and mitigate adverse events of mRNA-based therapies. Dr. McCullough said that some siRNAs [pitirosan and incleanseran] are already used in practice and that he hopes that a biological technology company will produce RIBOTAC.
Dr. McCullough recommends his Base Spike Protein Detoxification protocol that includes nattokinase, bromelin, and curcumin that are available at the Wellness Company He said that nattokinase dissolves blood clots and gave dosages in the video.
mRNA from the jabs has been shown to circulate in the blood for at least 28 days and can be stuck in lymph nodes for at least two months. Spike proteins are said to be circulating at high levels, based on antibodies against the spike protein.
Moderna has had several more mRNA ‘vaccines’, including one for the flu, approved. More mRNA injections will make people more progressively sick because it is synthetic and resistant to the body breaking it down naturally.
.
A preprint study coauthored by Dr. Peter McCullough, published in May, described a novel method of deactivating the genetic alteration effects of the mRNA Covid vaccinations, providing hope to the billions of people who’ve been genetically mutated.
“The Pfizer-BioNTech and Moderna biodistribution studies refute the assertion that nanolipid-bound nms-mRNA remains in the deltoid muscle or axillary lymph nodes. Detectable vaccine mRNA levels remaining in various tissues raises potential safety concerns,” the study said in the ‘Conclusions’ section. “The possibility of vaccine mRNA integration into the host genome and the prospect of unintended protein production due to read through advocate for a mechanism to eliminate lingering synthetic mRNA and halt damaging Spike protein production. The use of siRNA and RIBOTACs to target and degrade vaccine mRNA are promising approaches to mitigate deleterious health effects. The ability to readily tailor the siRNA and RIBOTACs to target an mRNA of interest makes these techniques particularly appealing, although further investigation is warranted to address challenges which include possible off-target effects and immune system activation.”
Messenger RNA (mRNA) technology, referred to in Moderna’s patents as modified mRNA or mmRNA for modified messenger RNA, is an exotic technology that encapsulates an altered RNA sequence within a lipid nanoparticle so as to introduce it into the cells of the vaccinated individual. The foreign man-made sequence is then incorporated into the cells of the vaccinated individual, thus acting more as a gene therapy than a traditional vaccine.
While the exotic injection makes the individual begin to produce the dangerous Covid spike protein, currently there is no way to stop the individual from producing that spike protein forever. There is no ‘off’ switch, at least until now.
The study described a method of turning off the production of the spike protein.
“…the longevity of the encapsulated mRNA along with unlimited production of the damaging and potentially lethal Spike (S) protein call for strategies to mitigate potential adverse effects,” the study said in the ‘Abstract’ section. “Here, we explore the potential of small interfering RNA (siRNA) and ribonuclease targeting chimeras (RIBOTACs) as promising solutions to target, inactivate, and degrade residual and persistent vaccine mRNA, thereby potentially preventing uncontrolled Spike protein production and reducing toxicity. The targeted nature of siRNA and RIBOTACs allows for precise intervention, offering a path to prevent and mitigate adverse events of mRNA-based therapies.”
Mounting research suggests a serious side effect of the COVID mRNA jabs could be dementia, and the prions that cause it may be contagious
Frameshifting, as we now know occurs in the COVID shots, can induce prion production and lead to neurodegenerative diseases such as Alzheimer’s and Creutzfeldt-Jakob disease (CJD)
Sid Belzberg’s prions.rip website, which collected data on neurological side effects post-jab, found a notably high incidence of diagnosed CJD cases, suggesting an alarming trend
A series of articles highlight biases in clinical trials and observational studies, suggesting COVID-19 vaccines’ safety and effectiveness have been massively overstated
The Global COVID Vaccine Safety Project study — funded by the U.S. Centers for Disease Control and Prevention — reveals significant side effects, including myocarditis, pericarditis, and blood clots, underscoring the need for reevaluation of COVID vaccine risks and benefits
According to mounting data, one of the more serious side effects of the COVID mRNA jabs appears to be dementia, and worse yet, this previously untransmissible disease may now be “contagious,” transmissible by way of prions.
In my 2021 interview with Stephanie Seneff, Ph.D., she explained why she suspected the COVID shots may eventually result in an avalanche of neurological prion-based diseases such as Alzheimer’s. She also published a paper detailing those mechanisms in the May 10, 2021, issue of the International Journal of Vaccine Theory. As she explained in that paper:1
“A paper published by J. Bart Classen (2021) proposed that the spike protein in the mRNA vaccines could cause prion-like diseases, in part through its ability to bind to many known proteins and induce their misfolding into potential prions.
Idrees and Kumar (2021) have proposed that the spike protein’s S1 component is prone to act as a functional amyloid and form toxic aggregates … and can ultimately lead to neurodegeneration.”
In summary, the take-home from Seneff’s paper is that the COVID shots, offered to hundreds of millions of people, are instruction sets for your body to make a toxic protein that will eventually wind up concentrated in your spleen, from where prion-like protein instructions will be sent out, leading to neurodegenerative diseases.
What Are Prions?
The term “prion” derives from “proteinaceous infectious particle.” Prions are known to cause a variety of neurodegenerative diseases in animals and humans, such as Creutzfeldt-Jakob disease (CJD) in humans, bovine spongiform encephalopathy (BSE or “mad cow disease”) in cattle, and chronic wasting disease in deer and elk.
These diseases are collectively referred to as transmissible spongiform encephalopathies (TSEs). They’re characterized by long incubation periods, brain damage, the formation of holes in the brain giving it a sponge-like appearance, and failure to induce an inflammatory response.
In short, prions are infectious agents composed entirely of a protein material that can fold in multiple, structurally distinct ways, at least one of which is transmissible to other prion proteins, leading to a disease that is similar to viral infections but without nucleic acids.
Unlike bacteria, viruses, and fungi, which contain nucleic acids (DNA or RNA) that instruct their replication, prions propagate by transmitting their misfolded protein state to normal variants of the same protein.
According to the prion disease model, the infectious properties of prions are due to the ability of the abnormal protein to convert the normal version of the protein into the misfolded form, thereby setting off a chain reaction that progressively damages the nervous system.
Prions are remarkably resistant to conventional methods of sterilization and can survive extreme conditions that would normally destroy nucleic acids or other pathogens, which is part of why prion diseases are so difficult to treat.
More Evidence mRNA Shots Can Trigger Dementia
Today, there’s even more evidence to support Seneff’s theory. In August 2022, tech entrepreneur Sid Belzberg wrote2 about prions.rip, a website he’d set up to collect data on the neurological side effects of the jabs. (This site is no longer live.)
Within a few months, the site had received about 15,000 hits and gathered 60 reports from people who got the jab and suffered neurological deficits shortly thereafter, including six cases of diagnosed CJD.
“Normally this disease affects 1 in a 1,000,000 people,” Belzberg wrote.3“To get 6 cases you would need 6,000,000 hits to the site assuming everyone reports. The chances of getting 1 case in 15,000 hits is 1 in 66. To see 6 cases in 1 group of 15,000 is 1/66^6 or 1 in 82,000,000,000, or 20 times more likely to win a Powerball lottery! …
To reiterate, CJD is an exceptionally rare disease that is now a known and established severe adverse reaction (SAE) from the DEATHVAX™. Injecting this slow kill bioweapon can cause ailments that are about as likely to develop in the real word as getting struck by lightning twice. The proof is now irrefutable.”
Frameshifting Can Result in Prion Production
In mid-December 2023, researchers reported4,5,6 that the replacing of uracil with synthetic methylpseudouridine in the COVID shots — a process known as codon optimization — can cause frameshifting, a glitch in the decoding, thereby triggering the production of off-target aberrant proteins.
The antibodies that develop as a result may, in turn, trigger off-target immune reactions. According to the authors, off-target cellular immune responses occur in 25% to 30% of people who have received the COVID shot. But that’s not all.
According to British neuroscientist Dr. Kevin McCairn, this frameshifting phenomenon has also been linked to harmful prion production — and that frame shifted prions, specifically, are infectious and can be transmitted from one person to another. As reported in the Journal of Theoretical Biology in 2013:7
“A quantitatively consistent explanation for the titres of infectivity found in a variety of prion-containing preparations is provided on the basis that the etiological agents of transmissible spongiform encephalopathy comprise a very small population fraction of prion protein (PrP) variants, which contain frameshifted elements in their N-terminal octapeptide-repeat regions …
Frameshifting accounts quantitatively for the etiology of prion disease. One per million frameshifted prions may be enough to cause disease. The HIV TAR-like element in the PRNP mRNA is likely an effector of frameshifting.”
McCairn explained this mechanism in a February 19, 2023, interview with Health Alliance Australia (video above). In it, he noted:
“Mis-folded proteins caused by prions can impact every level organ and tissue system in the body … [They] bioaccumulate and are resistant to degradation, thereby building up …”
Prions may in fact be the primary molecule that is being “shed” by COVID jab recipients, and if those prions are due to frameshifting, that could be very bad news indeed, considering their implication in dementia.
Another doctor who believes we’ll be facing an “epidemic of prion disease” is Dr. David Cartland. In late February 2024, he posted8 13 scientific papers linking the COVID jabs, prion diseases and CJD, noting that was just a “small selection” of what’s available in the medical literature.
Prions Implicated in Long COVID as Well
According to genomics expert Kevin McKernan, Ph.D., prions are also involved in long COVID (or as McKernan calls it, “long vax”).9 In one 2024 study,10 96.7% of long COVID sufferers had received the jab. In an interview with the Front Line COVID-19 Critical Care Alliance (FLCCC), McKernan stated:11
“If you frameshift over the stop codons, you’re going to be making proteins that are spike-mito proteins. When I talk to a lot of the long vax patients I hear of all these things that remind me of my time in the mitochondrial disease sequencing space …”
McKernan claims he tried to publish a paper on this in 2021 with Dr. Peter McCullough, but the editor of the journal “stepped in and torpedoed the paper.”12
World’s Largest Side Effect Analysis Has Been Published
In related news, the largest study13 to date on the side effects of the COVID jabs was published in the journal Vaccine in February 12, 2024, and it confirms what I and many other alternative news sources have been saying all along, namely that the mRNA jabs are the most dangerous medical products to ever hit the market.
The study — performed by the Global COVID Vaccine Safety (GCoVS) Project and funded by the U.S. Centers for Disease Control and Prevention, Public Health Ontario and the Canadian Health Research Institute — evaluated the risk of “adverse events of special interest” (AESI) following COVID-19 “vaccination.”
Data from 10 sites in eight countries (Argentina, Australia, Canada, Denmark, Finland, France, New Zealand and Scotland) were included, encompassing more than 99 million jabbed individuals.
Of the thousands of side effects Pfizer listed in its confidential report of post-authorization adverse events submitted to the U.S. Food and Drug Administration,14 the GCoVS focused on 13 AESIs that fall into three primary categories: Neurological, hematologic (blood-related) and cardiovascular conditions.
They calculated the AESI risk for each of the 13 AESIs based on the number of observed versus expected (OE) incidents occurring up to 42 days after injection. The “expected” number of side effects were based on vaccine adverse event data from 2015 to 2019. These rates were then compared to the adverse event rates observed in those who got one or more of the COVID jabs, either Pfizer’s BNT162b2, Moderna’s mRNA-1273, or AstraZeneca’s ChAdOx1.
Largest Study to Date Confirms COVID Jab Dangers
The analysis15 revealed several concerning side effects, including increased risks of myocarditis, pericarditis, blood clots in the brain, and various neurological conditions. Here’s a quick summary of the findings:
•Myocarditis and pericarditis:
◦Pfizer vaccine — OE ratios for myocarditis were 2.78 and 2.86 after the first and second shots, with the risk remaining doubled after the third and fourth shots.
◦Moderna vaccine — OE ratios for myocarditis were 3.48 and 6.10 after the first and second shots. Doses 1 and 4 also showed OE ratios of 1.74 and 2.64 for pericarditis.
◦AstraZeneca vaccine — OE ratio for pericarditis was 6.91 after the third shot.
•Blood clots in the brain (cerebral venous sinus thrombosis, CVST):
◦An OE of 3.23 for CVST was observed after the first AstraZeneca shot.
◦A significant increase in CVST risk was also noted after the second Pfizer dose.
•Neurological conditions:
◦Guillain-Barré syndrome — An OE ratio of 2.49 was observed following the AstraZeneca jab.
◦Transverse myelitis — Risk nearly doubled with the AstraZeneca shot.
◦Acute disseminated encephalomyelitis — OE ratios of 3.78 (Moderna) and 2.23 (AstraZeneca) were noted.
These findings really underscore the potential for serious side effects from the COVID shots, including conditions that may lead to other consequences in the longer term, such as stroke, heart attack, paralysis and death.
Effectiveness and Safety Was Wildly Exaggerated in Trials
Considering those findings, it’s no surprise to find that effectiveness and safety were exaggerated in clinical trials and observational studies. In a guest post on Dr. Robert Malone’s Substack, Raphael Lataster, Ph.D., writes:16
“An unofficial series of four crucially important medical journal articles, two by me, appearing in major academic publisher Wiley’s Journal of Evaluation in Clinical Practice reveals that claims made about COVID-19 vaccines’ effectiveness and safety were exaggerated in the clinical trials and observational studies, which significantly impacts risk-benefit analyses.
Also discussed are the concerning topics of myocarditis, with evidence indicating that this one adverse effect alone means that the risks outweigh the benefits in the young and healthy; and perceived negative effectiveness, which indicates that the vaccines increase the chance of COVID-19 infection/hospitalization/death, to say nothing about other adverse effects.”
Summary of Papers
The four papers in question include:
1.“Sources of Bias in Observational Studies of COVID-19 Vaccine Effectiveness” published in the Journal of Evaluation in Clinical Practice in March 2023, co-authored by BMJ editor Peter Doshi, Ph.D., statistician Kaiser Fung and biostatistician Mark Jones, which concluded that “case-counting window bias” had a significant effect on effectiveness estimates.17
As explained by Lataster, this “concerns the 7 days, 14 days, or even 21 days after the jab where we are meant to overlook jab-related issues, such as COVID infections, for some odd reason as ‘the vaccine has not had sufficient time to stimulate the immune system.’
This may strike you as quite bizarre since all of the ‘fully vaccinated’ must go through the process of being ‘partially vaccinated,’ sometimes even more than once. To make matters worse, the unvaccinated do not get such a ‘grace period,’ meaning that there is also a clear bias at play.
In an example using data from Pfizer’s clinical trial, the authors show that thanks to this bias, a vaccine with effectiveness of 0%, which is confirmed in the hypothetical clinical trial, could be seen in observational studies as having effectiveness of 48%.”
2.“Reply to Fung et. al. on COVID-19 Vaccine Case-Counting Window Biases Overstating Vaccine Effectiveness,” authored by Lataster, which discussed how the counting window bias not only affected effectiveness estimates in observational studies but also safety estimates, suggesting a need for reassessment of vaccine safety.18 The article also addresses “the mysterious rise in non-COVID excess deaths post-pandemic.”19
3.“How the Case Counting Window Affected Vaccine Efficacy Calculations in Randomized Trials of COVID-19 Vaccines,” again co-authored by Doshi and Fung, which detailed how case-counting window issues also overestimated effectiveness in Pfizer and Moderna clinical trials.20
4.A second article by Lataster, in which he highlighted and summarized the evidence showing that clinical trials were affected by adverse effect counting window issues that led to exaggerated safety estimates.21
“Together, these four articles make clear that claims made about COVID-19 vaccines; effectiveness and safety were exaggerated in the clinical trials and observational studies, whilst also finding time to discuss myocarditis and perceived negative effectiveness, meaning that new analyses are very much needed,” Lataster writes.22
Resources for Those Injured by the COVID Jab
Based on data from across the world, it’s beyond clear that the COVID shots are the most dangerous drugs ever deployed. If you already got one or more COVID jabs and are now reconsidering, you’d be wise to avoid all vaccines from here on, as you need to end the assault on your body. Even if you haven’t experienced any obvious side effects, your health may still be impacted long-term, so don’t take any more shots.
If you’re suffering from side effects, your first order of business is to eliminate the spike protein — and/or any aberrant off-target protein — that your body is producing. Two remedies shown to bind to and facilitate the removal of SARS-CoV-2 spike protein are hydroxychloroquine and ivermectin. I don’t know if these drugs will work on off-target proteins and nanolipid accumulation as well, but it probably wouldn’t hurt to try.
The Front Line COVID-19 Critical Care Alliance (FLCCC) has developed a post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com.23
For additional suggestions, check out the World Council for Health’s spike protein detox guide,24 which focuses on natural substances like herbs, supplements and teas. Sauna therapy can also help eliminate toxic and misfolded proteins by stimulating autophagy.
Tennessee Lawmakers Pass Bill Targeting mRNA Vaccines In Food
Following concerns over research to embed vaccines in produce, the Tennessee Senate has passed a bill which would require any food containing vaccines or vaccine materials to be labeled as pharmaceutical drugs.
Lettuce grows under artificial lights on an automated growing rack at a farm in Nottingham, Maryland, on April 14, 2023.
The bill, HB 1894, was passed by the Senate in a 23-6 vote on March 28 after the state House passed it 73-22 on March 4. It awaits the governor’s signature.
The bill comes in response to a University of California-Riverside research project looking into whether mRNA which targets pathogens could be implanted into edible plants, which would then be consumed. The research was funded by a $500,000 grant from the National Science Foundation.
“You would have to get a prescription for that to make sure that we know how much of the lettuce you have to eat based off of your body type so we don’t under-vaccinate you, which leads to the possibility of the efficacy of the drug being compromised, or we overdose you based off how much lettuce is [eaten],” said Republican state Rep. Scott Cepicky during a House committee meeting in February, WKRN-TV reports.
Cepicky said that the bill, which local media described as a move targeting “vaccine lettuce,” would classify foods modified to act as vaccines, as pharmaceuticals.
“So if you want to consume them you would go to your doctor and get a prescription,” he said.
In a 2021 press release, UC Riverside associate professor of Botany and Plant Sciences, Juan Pablo, said “We are testing this approach with spinach and lettuce and have long-term goals of people growing it in their own gardens,” adding “Farmers could also eventually grow entire fields of it.”
According to Pablo, “Ideally, a single plant would produce enough mRNA to vaccinate a single person.”
Another researcher, Nicole Steinmetz, said in the same release that they planned to use nanoparticles or “plant viruses, for gene delivery to plants.”
When asked by WKRN-TV about the status of the research, a UC Riverside spokesperson said that the project is not yet complete.
“Research into the process of having plant chloroplasts express vaccine chemistry is ongoing. There are no definitive results to report,” said Jules Berinstein after the Tennessee bill was passed.
Democrat Senators oppose
During the debate on the Tennessee Senate Floor, some lawmakers questioned the need for the bill.
“Does the sponsor know of any instances of there being food offered in the state of Tennessee that contains vaccines in some kind of a retail or public forum?” asked state Sen. Heidi Campbell.
Rep. Cepicky hit back, highlighting in February that a Kentucky company has already been “infecting growing tobacco plants with a genetically modified coronavirus” to see if it can produce antibodies for a potential vaccine, adding that the company “can already do this right now.”
Massie sounds the alarm
In 2023, US Rep. Thomas Massie (R-KY) raised concerns over the use of federal money to create “transgenic edible vaccines,” which would transform edible plants such as spinach and lettuce into mRNA vaccine delivery vehicles.
In September 2023 during a debate over an appropriations bill, Massie highlighted an incident in which an edible vaccine was introduced into a corn crop used to feed pigs in order to mitigate diarrhea. The corn crop, however, became commingled with a soybean crop – contaminating 500,000 bushels that had to be recalled.
“Do we want humans eating vaccines that were grown in corn meant to stop pigs from getting diarrhea? I don’t think we want that to happen. Yet that almost happened, and it could happen,” said Massie. “There is another case where the pollen cross-contaminated another crop of corn, and 155 acres of corn had to be burned. What are the cases where we’re not discovering this? I think it’s dangerous to play God with our food.”
The Department of Health and Human Services (HHS) was paying OB-GYN doctors millions of dollars to lie to mothers that COVID mRNA injections are safe. Naomi Wolf said that if the doctors tell the truth about the dangers of COVID injections, they will have to repay the money that they received. She said that they are criminals. She said that Pfizer is aware that babies died after their mothers received COVID jabs. She asserted that babies and unborn babies have been murdered.
Naomi Wolf, a researcher and the CEO of Daily Clout, said that the Department of Health and Human Services (HHS) was paying OB-GYN doctors millions of dollars to ‘stick to the script’ and to lie to mothers that COVID mRNA injections are safe. She said that if the doctors tell the truth about the dangers of COVID injections, they will have to repay the money that they received. Wolf called these doctors criminals.
She said that the American College of Obstetrics and Gynecology, a large lobbying group, had a portal where OB-GYN doctors could register to receive money directly fro HHS in 2020 if they attested that their patients had COVID as a primary diagnosis, or, if they were pregnant, COVID could be used as a secondary diagnosis. OB-GYN doctors were incentivized in 2020 to inflate COVID diagnosis numbers.
Wolf reported that maternal deaths are up 40% after COVID injections. She said that a doctor and midwives have told her that babies are being born prematurely, they are being born with fetal malformations, chromosomal malformations and breathing problems.
She said that babies and unborn have been murdered.
Wolf said that Pfizer documents reveal that they knew that two babies died in-utero and the vaccine manufacturer stated that the deaths were due to “trans-placental exposure” to the vaccine and then they sent that report to the CDC in April 10, 2021. Three days later, CDC head Rochelle Walensky gave a press conference from the White House stating that pregnant women should take the mRNA vaccines and that it was safe and effective at any time, before, during, or after pregnancy. Wolf said that Walensky knew that two babies had died from trans-placental exposure and another baby died from poisoned breast milk when she advised the women to take the COVID shots.
A new bill has been introduced in Idaho that would make the administration of experimental mRNA COVID-19 vaccines illegal.
Representative Judy Boyle (R-Midvale) and Senator Tammy Nichols (R-Middleton) sponsored House Bill 154.
Sen. Nichols introduced the new bill on the 15th of February before the House Health and Welfare Committee, according to KTVB.
According to the bill text, “A person may not provide or administer a vaccine developed using messenger ribonucleic acid technology for use in an individual or any other mammal in this state.”
Nichols said during her presentation to the committee, “We have issues this was fast tracked.”
Nichols said there is no liability, informed consent or data on mRNA vaccines. She later clarified she was referring to the two COVID-19 vaccines, Pfizer and Moderna.
“I think there is a lot of information that comes out with concerns to blood clots and heart issues,” Nichols said.
Rep. Ilana Rubel, D-Boise, questioned Nichols’ statement that the vaccines were fast-tracked. She said her understanding was that the vaccines were approved and survived the testing, later approved by the FDA.
Nichols said she is finding it “may not have been done like we thought it should’ve been done.”
“There are other shots we could utilize that don’t have mRNA in it,” Nichols said.
More and more medical experts, scientists, and right group advocates all over the world are now demanding that the government should stop its COVID-19 vaccination campaign due to its devastating side effects among patients.
And yet governments still turn a blind eye to one of the most atrocious crimes against humanity.
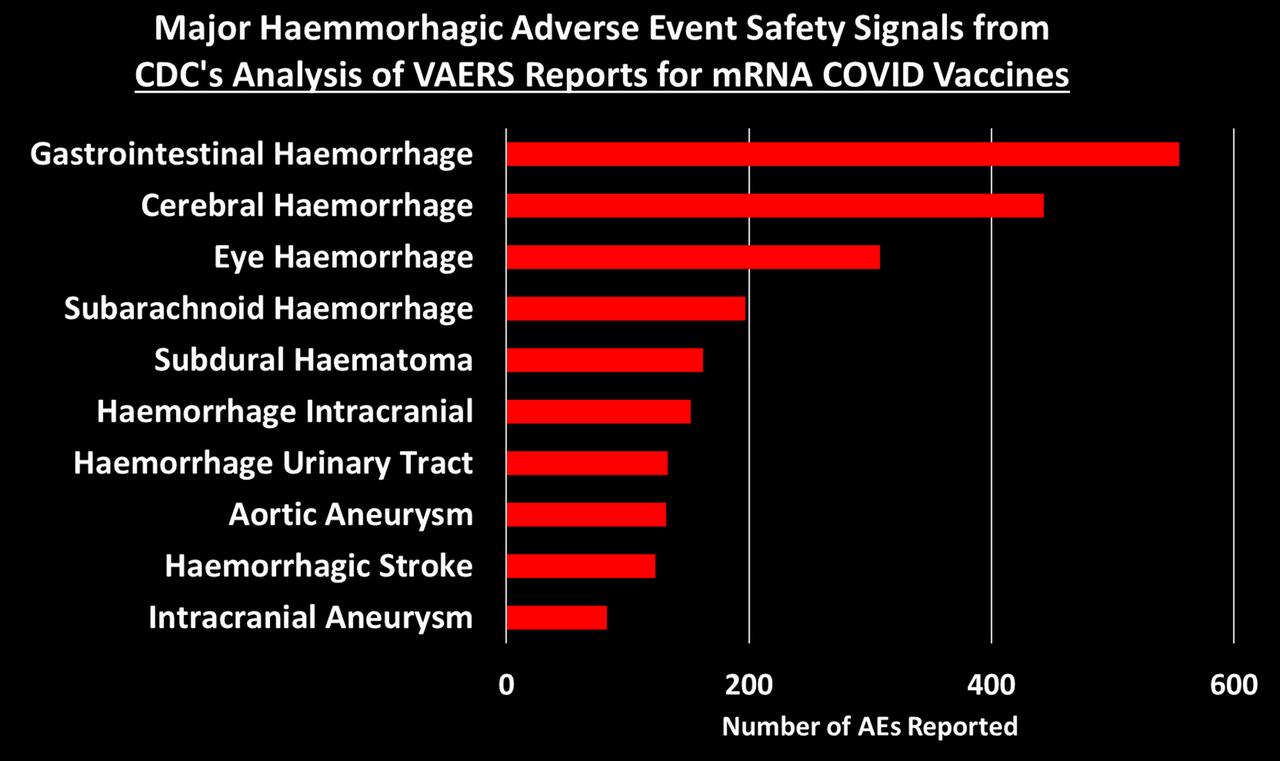
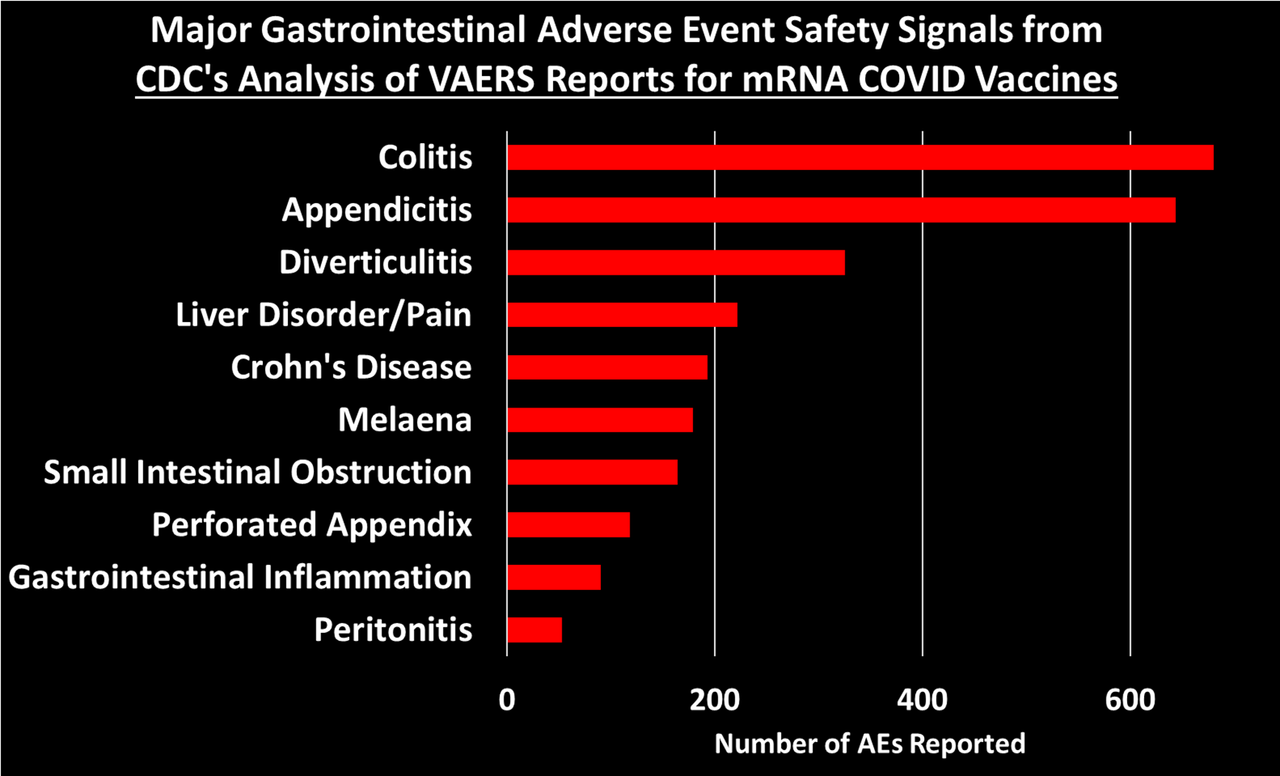
CDC’s VAERS safety signal analysis based on reports from Dec. 14, 2020 – July 29, 2022 for mRNA COVID-19 vaccines shows clear safety signals for death and a range of highly concerning thrombo-embolic, cardiac, neurological, hemorrhagic, hematological, immune-system and menstrual adverse events (AEs) among U.S. adults.
There were 770 different types of adverse events that showed safety signals in ages 18+, of which over 500 (or 2/3) had a larger safety signal than myocarditis/pericarditis.
The CDC analysis shows that the number of serious adverse events reported in less than two years for mRNA COVID-19 vaccines is 5.5 times larger than all serious reports for vaccines given to adults in the US since 2009 (~73,000 vs. ~13,000).
Twice as many mRNA COVID-19 vaccine reports were classified as serious compared to all other vaccines given to adults (11% vs. 5.5%). This meets the CDC definition of a safety signal.
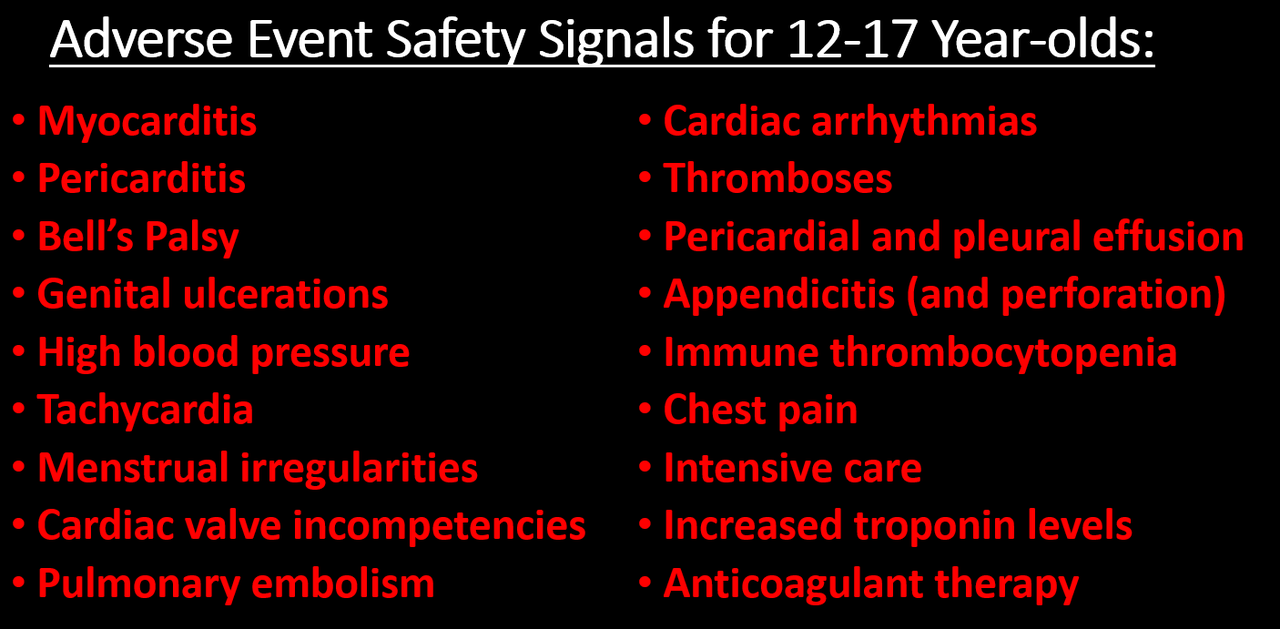
There are 96 safety signals for 12-17 year-olds, which include: myocarditis, pericarditis, Bell’s Palsy, genital ulcerations, high blood pressure and heartrate, menstrual irregularities, cardiac valve incompetencies, pulmonary embolism, cardiac arrhythmias, thromboses, pericardial and pleural effusion, appendicitis and perforated appendix, immune thrombocytopenia, chest pain, increased troponin levels, being in intensive care, and having anticoagulant therapy.
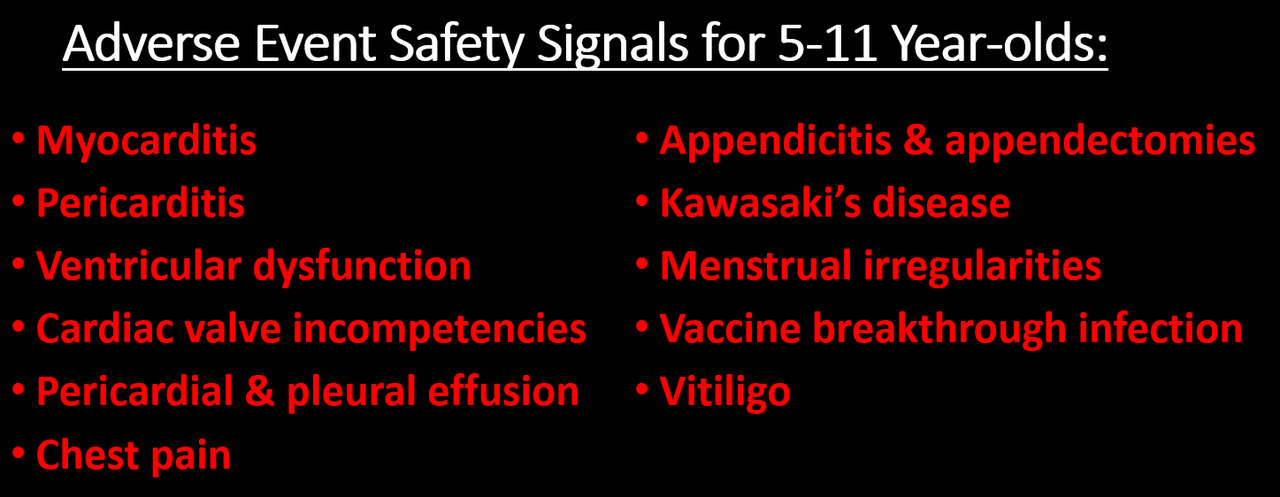
There are 66 safety signals for 5-11 year-olds, which include: myocarditis, pericarditis, ventricular dysfunction and cardiac valve incompetencies, pericardial and pleural effusion, chest pain, appendicitis & appendectomies, Kawasaki’s disease, menstrual irregularities, vitiligo, and vaccine breakthrough infection.
The safety signals cannot be dismissed as due to “stimulated,” exaggerated, fraudulent or otherwise artificially inflated reporting, nor can they be dismissed due to the huge number of COVID vaccines administered. There are several reasons why, but the simplest one is this: the safety signal analysis does not depend on the number of reports, but whether or not some AEs are reported at a higher rate for these vaccines than for other non-COVID vaccines. Other reasons are discussed in the full post below.
In August, 2022, the CDC told the Epoch Times that the results of their safety signal analysis “were generally consistent with EB [Empirical Bayesian] data mining [conducted by the FDA], revealing no additional unexpected safety signals.” So either the FDA’s data mining was consistent with the CDC’s method—meaning they “generally” found the same large number of highly alarming safety signals—or the signals they did find were expected. Or they were lying. We may never know because the FDA has refused to release their data mining results.
INTRODUCTION
Finally! Zachary Stieber at the Epoch Times managed to get the CDC to release the results of its VAERS safety signal monitoring for COVID-19 vaccines, and they paint a very alarming picture (see his reporting and the data files here, or if that is behind a paywall then here). The analyses cover VAERS reports for mRNA COVID vaccines from the period from the vaccine rollout on December 14, 2020 through to the end of July, 2022. The CDC admitted to only having started its safety signal analysis on March 25, 2022 (coincidentally 3 days after a lawyer at Children’s Health Defense wrote to them reminding them about our FOIA request for it).
[UPDATE: T Coddington left a link in comments to a website where he made the data in the Excel files more accessible.]
Like me, you might be wondering why the CDC waited over 15 months before doing its first safety signal analysis of VAERS, despite having said in a document posted to its website that it would begin in early 2021—especially since VAERS is touted as our early warning vaccine safety system. You might also wonder how they could insist all the while that the COVID-19 vaccines are being subjected to the most rigorous safety monitoring the world has ever known. I’ll come back to that later. First I’m going to give a little background information on the analysis they did (which you can skip if you’re up to speed) and then describe what they found.
BACKGROUND ON SAFETY SIGNAL ANALYSIS
Back in June 2022, the CDC replied to a Freedom of Information Act (FOIA) request for the safety signal monitoring of the Vaccine Adverse Events Reporting System (VAERS)—the one it had said it was going to do weekly beginning in early 2021. Their response was: we never did it. Then a little later they said they had been doing it from early on. But by August, 2022, they had finally gotten their story straight, saying that they actually did do it, but only from March 25, 2022 through end of July. You can get up to speed on that here.
The analysis they were supposed to do uses what’s called proportional reporting ratios (PRRs). This is a type of disproportionality analysis commonly used in pharmacovigilance (meaning the monitoring of adverse events after drugs/vaccines go to market). The basic idea of disproportionality analysis is to take a new drug and compare it to one or more existing drugs generally considered safe. We look for disproportionality in the number of adverse events (AEs) reported for a specific AE out of the total number of AEs reported (since we generally don’t know how many people take a given drug). We then compare to existing drugs considered safe to see if there is a higher proportion of particular adverse events reported for the new drug compared to existing ones. (In this case they are looking at vaccines, but they still use PRR even though they generally have a much better sense of how many vaccines were administered.)
There are many ways to do disproportionality analysis. The PRR is one of the oldest. Empirical Bayesian data mining, which was supposed to be done on VAERS by the FDA, is another. The PRR is calculated by taking the number of reports for a given adverse event divided by the total number of events reported for the new vaccine or the total number of reports. It then divides that by the same ratio for one or more existing drugs/vaccines considered safe. Here is a simple formula:
So for example, if half of all adverse events reported for COVID-19 vaccines and the comparator vaccine(s) are for myocarditis, then the PRR is 0.5/0.5 = 1. If one quarter of all AEs for the comparator vaccine are for myocarditis, then the PRR is 0.5/0.25 = 2.
Traditionally, for a PRR to count as a safety signal, the PRR has to be 2 or greater, have a Chi-square value of 4 or greater (meaning it is statistically significant) and there has to be at least 3 events reported for a given AE. (This also means that if there are tons of different AEs reported for COVID vaccines that have never been reported for any other vaccine, it will not count as a safety signal. I found over 6,000 of those in my safety signal analysis from 2021.
Ah yes, shared with the public — after first refusing to share the results and months of foot-dragging following repeated FOIA requests! We will see that the CDC has not done a more focused study on almost any of adverse events with “new patterns” (AKA safety signals).
SO WHAT DID THE CDC ACTUALLY DO?
The Epoch Times obtained 3 weeks of safety signal analyses from the CDC for VAERS data updated on July 15, 22 and 29, 2022. Here I will focus on the last one, since there is very little difference between them and it is more complete. The safety signal analysis compares adverse events1 reported to VAERS for mRNA COVID-19 vaccines from Dec. 14, 2020 through July 29, 2022 to reports for all non-COVID vaccines from Jan 1, 2009 through July 29, 2022.
PRRs are calculated separately for 5-11 year-olds, 12-15 year-olds and 18+ separately. For each age group, there are separate tables for AEs from all reports, AEs from reports marked serious and AEs from reports not marked as serious.2 Recall that a serious report is one that involves death, a life-threatening event, new or prolonged hospitalization, disability or permanent damage, or a congenital anomaly. I will focus on the reports for all AE’s.
They also have a table that calculates PRRs by comparing reports for the Pfizer COVID-19 vaccine to reports for the Moderna vaccine and vice versa, again for all reports, serious reports only and non-serious reports. There were no remarkable findings in those tables, so I will not discuss them. [Edit: I forgot what Norman Fenton noted in his analysis: the overall proportion of reports with serious adverse events is 9.6% for Modern compared to 12.6% for Pfizer.] This isn’t that surprising since both vaccines are very similar and so should present relatively similar adverse events when compared to each other, and any differences are likely not large enough to be picked up by a PRR analysis. [Though the difference in the overall rate of serious adverse events, which are not specific to a particular type of event only how serious it is, was significant.]
The CDC seems to have calculated PRRs for every different type of adverse event reported for all the COVID vaccines examined – though it’s possible they only analyzed a subset. What seems clear is that, among the AEs they examined, the only ones included in the tables satisfy at least one of two conditions: a PRR value of at least 2 and a Chi-square value of at least 4 (Chi is the Greek letter χ and is pronounced like ‘kai’). When both conditions were met, they highlighted the adverse event in yellow, which appears to indicate a safety signal. There were no COVID vaccine AEs listed with fewer than 3 reported events, though for non-COVID vaccines there were many AEs listed that had only 1 or 2 reported since 2009. The CDC tables still include these and highlight them in yellow when the PRR is greater than 2 and the Chi-square value is great than 4, indicating these events are counted as safety signals.
WHAT SAFETY SIGNALS DID THE CDC FIND?
I’m going to divide this up by age groups and the Pfizer v. Moderna comparison. Let’s start with the 18+ group.
There are 772 AEs that appear on the list. Of these, 770 are marked in yellow and have PRR and Chi-square values that qualify them as safety signals. Some of these are new COVID-19 related codes, and we would expect those to trigger a signal since they didn’t exist in prior years to be reported by other vaccines. So if we take those off, we are left with 758 different types of non-COVID adverse events that showed safety signals.
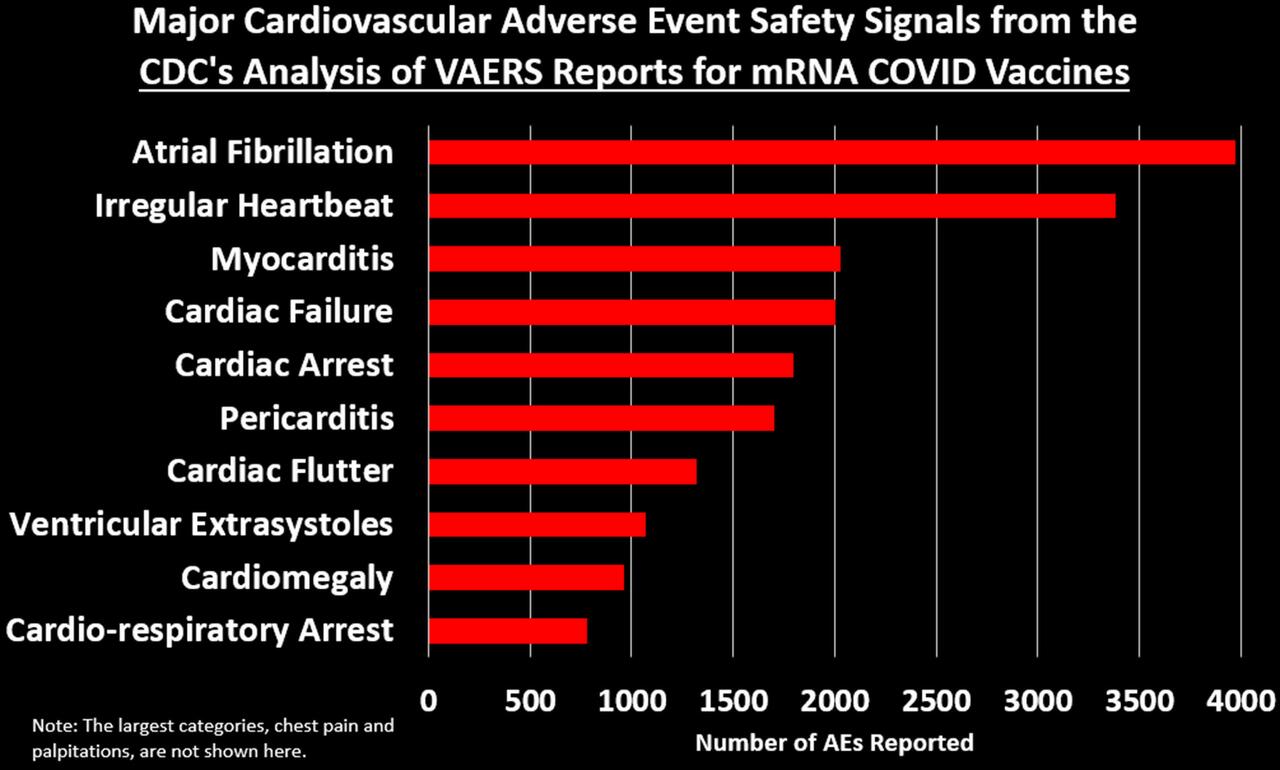
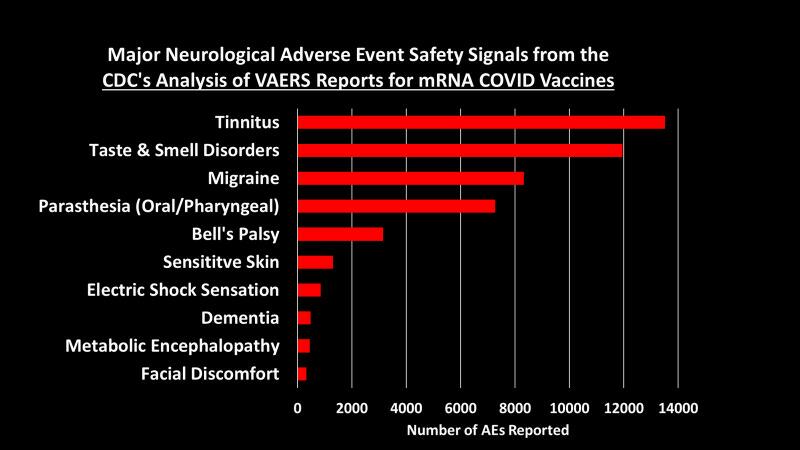
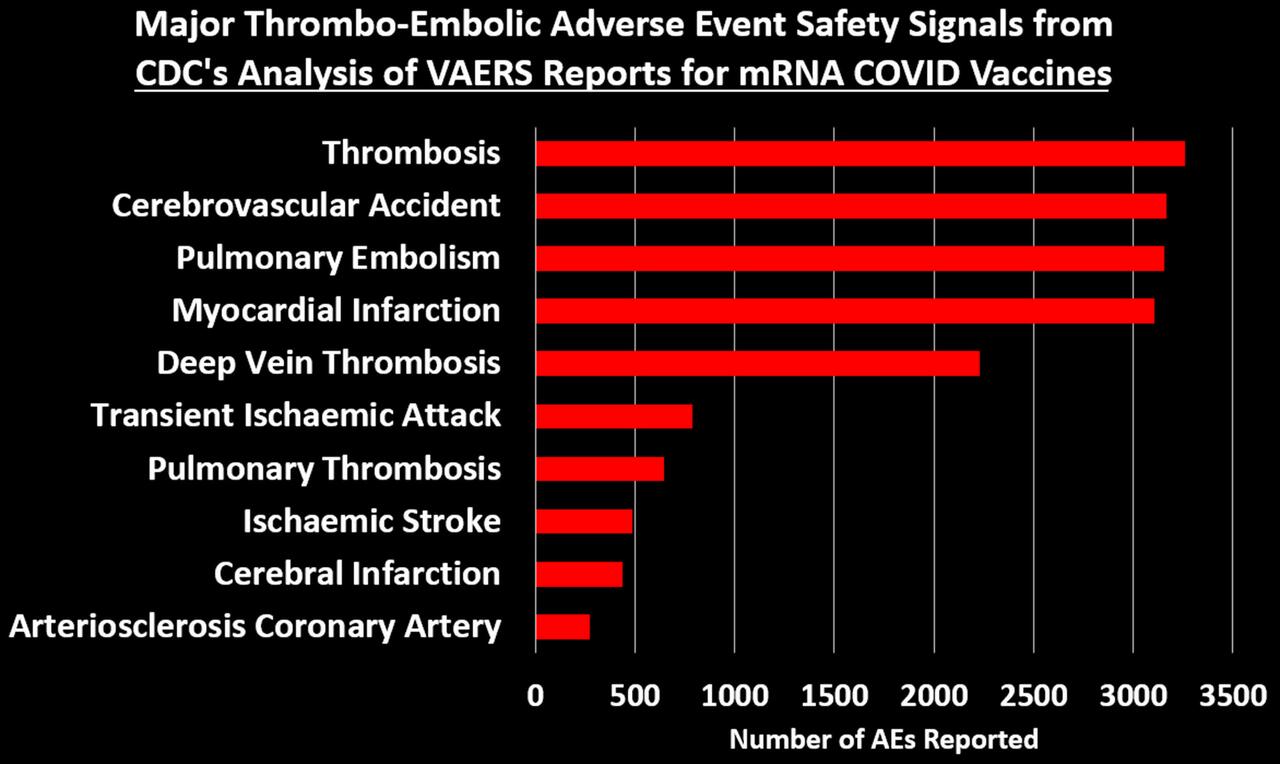
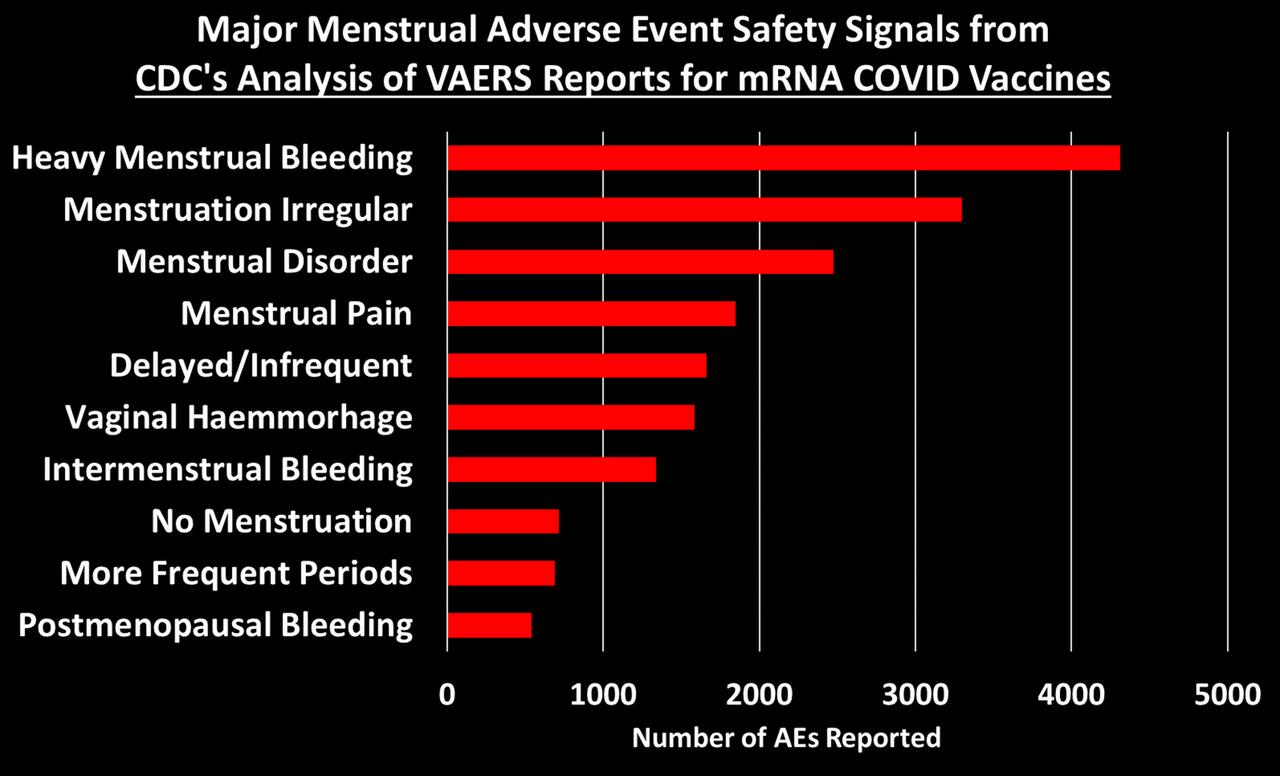
I grouped these 758 safety signals into different categories. The figure below shows the total number of AEs reported for each of the major categories of safety signals:
Let’s dig into some of these categories to look at what types of AEs generated the most number of reports:3
Let’s dig into some of these categories to look at what types of AEs generated the most number of reports:3
You can peruse the adverse events using the Excel tables provided by the CDC, which were posted by The Epoch Times and Children’s Health Defense at the links at the top of this post.
What about The Children?
If there is anything that looks remotely like a bright spot in all of this is that the list of safety signals for 12-17 and 5-11 year-olds is much shorter than for 18+. There are 96 AEs that qualify as a safety signal for the 12-17 group and 67 for the 5-11. When we take out the new COVID-era AEs, there are 92 safety signals for 12-17 year-olds and 65 for 5-11 year-olds. Here are the most alarming ones:
I don’t know why the list of AE’s is so much shorter for these age groups. It could be that the list of AE’s for other vaccines for these age groups is much shorter, so in a case where AEs have been reported for the mRNA COVID vaccines but not for other vaccines, it will not be counted as a safety signal by definition.
COMPARISONS TO MYOCARDITIS & PERICARDITIS
We are told that the existence of a safety signal doesn’t necessarily mean the AE is caused by the vaccine, and I accept that premise. But the current practice seems to be to ignore safety signals, dismiss them as noise without any evidence, and stall any investigation into them as long as possible. The precautionary principle, however, dictates we should presume that a safety signal indicates causality, until proven otherwise. Since, it has been acknowledged that the mRNA COVID vaccines can cause myocarditis and pericarditis (often referred to as myo-pericarditis), we can take those AEs as a kind of benchmark, and propose that, at minimum, any AE with a signal of equal or greater size should be considered potentially causal and investigated more thoroughly.4
After dropping the new COVID-era AEs, there are 503 AEs with PRRs larger than myocarditis (PRR=3.09) and 552 with PRRs larger than pericarditis (PRR=2.82).5This means that 66.4% of the AEs had a bigger safety signal than myocarditis and 77.3% were larger than pericarditis. You can see what those were by use this Excel file provided by the CDC and sorting the 18+ tab by the 12/14-07/29 PRR column (Column E). Then just look at which AEs have PRRs larger than the ones for pericarditis and myocarditis.
For 12-17 year-olds, there is 1 safety signal larger than myocarditis (it’s ‘troponin increased’) and 14 safety signals larger than pericarditis (excluding myocarditis), which include: mitral valve incompetence, bell’s palsy, heavy menstrual bleeding, genital ulceration, vaccine breakthrough infection, and a range of indicators of cardiac abnormalities.
For 5-11 year-olds, the comparison to myo/pericarditis is less germane, as they seem to suffer less from this side effect. But we can still make the comparison: there are 7 safety signals larger than pericarditis, including bell’s palsy, left ventricular dysfunction, mitral valve incompetence, and ‘drug ineffective’ (presumably meaning they still got COVID). There are 16 safety signals larger than myocarditis (excluding pericarditis), which in addition to those listed above also include: pericardial effusion, diastolic blood pressure increase, tricuspid valve incompetence, and vitiligo. Sinus tachycardia (high heart rate), appendicitis, and menstrual disorder come in just below myocarditis.
Now if we think of a safety signal as having both strength and clarity, then the PRR can be thought of as an indicator of how strong the signal is, while the Chi-square is a measure of how clear or unambiguous the signal is, because it gives us a sense of how likely the signal is due to chance alone: the larger the Chi-square value, the less likely the signal is due to chance. A Chi-square of 4 means there is only a 5% chance the observed signal is due to chance. A Chi-square of 8 means there is only a 0.5% chance of it being due to chance.6
For the 18+ group, there are 57 AEs with a Chi-square larger than myocarditis (Chi-square=303.8) and 68 with a Chi-square larger than pericarditis (Chi-square=229.5). Again, you can see what these are by going the Excel file linked above and sorting on Column D.
For the 12-17 group, there are 4 AEs with a larger Chi-square than myocarditis (Chi-square=681.5) and 6 larger than pericarditis (Chi-square=175.4).
For the 5-11 group, there are 22 AEs with a Chi-square larger than myocarditis (Chi-square=30.42) and 34 AEs with a Chi-square larger than pericarditis (Chi-square=18.86).
RESPONDING TO OBJECTIONS
Let’s dispense with some of the criticisms used to dismiss VAERS data, which will undoubtedly be raised if you try to bring the CDC’s analysis to people’s attention.
Objection: Anybody can report to VAERS. The reports are unreliable. Anti-vaxxers made lots of fraudulent reports. Nobody was aware of VAERS in the past, but now they are. So many people were afraid of the vaccine so they blamed all their health problems on it. Health workers were required by law to report certain adverse events, like deaths and anaphylaxis. Etc. Etc.
All of these objections ultimately rely on the notion that VAERS reports for COVID-19 vaccines have been artificially inflated over previous years for one reason or another. The thing of it is, though, that the CDC has a method for distinguishing between artificial inflation and real signal. The idea is simple: if adverse events are artificially inflated, they should be artificially inflated to the same degree. Meaning, the PRRs for all of these safety signals should be about the same. But even a casual glance at the PRRs in the Excel file show they vary widely, from as low at 2 to as high as 105 for vaccine breakthrough infection or 74 for cerebral thrombosis. This method does not on the number of reports, but the rate of reporting for certain events out of all events reported. If anything, this method would tend to hide safety signals in a situation where a new vaccine generates a very large number of reports.
The CDC has even done us the favor of calculating upper and lower confidence intervals, meaning that we can be at least 95% confident that two PRRs are truly different if their confidence intervals don’t overlap. So for example the lower confidence interval for pulmonary thrombosis is 19.7, which is higher than the upper confidence interval for 543 other signals. Artificially inflated reporting cannot explain why so many different adverse events have large PRRs that are statistically distinct from one another.
Objection: The safety signals are due to the huge number of COVID vaccines given out. Never before have we given out so many vaccine doses. By the end of July, the US had administered something like 600 million vaccine doses to people aged 18+. But the CDC analysis compares VAERS reports for these doses to all doses for all other vaccines for this age group since Jan. 1, 2009. But from 2015-2020 there were over 100 million flu doses administered annually to this age group alone. In previous work, I estimated 538 million doses of flu given to people 18+ from July 2015-June 2020. The number of flu and other non-COVID vaccines for this age group administered from Jan 1., 2009 through July 29, 2022 must be well over double this number, meaning VAERS reports for COVID vaccines are being compared to reports for at least double the number of doses for other vaccines. In addition to this, as already noted, the PRR methodology does not depend, strictly speaking, on the number of doses, but rather the rate of reporting of a specific AE out of all AEs for that vaccine.
Objection: the vaccines are mainly being given to older people who tend to have health problems, whereas other vaccines are given to younger people. This objection is dealt with, since the analyses are stratified by age groups. It might be still be somewhat valid for the 18+ group, except that in the safety signal analysis I did in the fall of 2021, I stratified by smaller age bands and still found safety signals. In any case, this objection is not enough to dismiss the safety signal analysis out of hand, but rather calls for better and more refined research.
Objection: The VAERS data is not verified and cannot be trusted. I’ll be the first person to agree that VAERS is not high quality data, but if it is completely untrustworthy, then how is it that the CDC uses these data to publish in the best medical journals such as JAMA and The Lancet? If the data were worthless, then these journals shouldn’t accept these papers. In that JAMA paper, they reported that 80% of the myocarditis reports met their definition of myocarditis and were included in the analysis. Many other reports simply needed more details for validation. Furthermore, the CDC has the ability and budget to follow-up on every report VAERS receives to get more details and even medical records to verify the report.
So if myocarditis shows a clear signal in the CDC’s analysis, and 80% of those reports were apparently high quality enough to be included in a paper published in one of the world’s top medical journals, how is it possible that all the rest of the reports are junk? That all of the other safety signals are meaningless? Answer: it isn’t.
And since we’re on the topic of safety signals that turned out to be real, it’s instructive to find appendicitis turn up as a safety signal in all 3 age groups, since a study published in NEJM based on medical records of over a million adult Israelis found an increased risk of appendicitis in the 42 days following Pfizer vaccination (but not following a positive SARS-CoV-2 PCR test). That study also found an increase in lymphadenopathy (swollen lymph nodes) after vaccination, but not after positive COVID test. Lymphadenopathy was another safety signal.
And that brings us to our last objection to be dispensed with: all of these AEs were due to COVID. There was an epidemic and so people were falling ill due to COVID and having all of these problems that were then blamed on the vaccine. Well to begin with, as we just saw, at least two of them (appendicitis and lymphadenopathy) do not appear to have increased risk ratios following a positive SARS-CoV-2 test, and we know that the mRNA vaccines increase risk of myo/pericarditis independent of infections. So how can we assume the rest of these are and dismiss them with the wave of a hand? We can’t. At minimum, they need further investigation. Furthermore, in the safety signal analysis I did in 2021, I dropped all VAERS reports where any sign of a SARS-CoV-2 exposure or infection was indicated on the report, and I still found large, significant safety signals.
PUTTING IT ALL INTO PERSPECTIVE
The Epoch Times article quotes my esteemed colleague and friend, Norman Fenton, Professor of Risk Management and an world renowned expert in Bayesian statistical analysis: “from a Bayesian perspective, the probability that the true rate of the AE of the COVID-19 vaccines is not higher than that of the non-COVID-19 vaccines is essentially zero…. The onus is on the regulators to come up with some other causal explanation for this difference if they wish to claim that the probability a COVID vaccine AE results in death is not significantly higher than that of other vaccines.” (See his post on the CDC analysis here.) The same is true for all the safety signals they found.
The CDC’s VAERS SOP analysis document lists 18 Adverse Events of Special Interest says they are going to pay close attention to. In their 2021 JAMA paper (and similar presentations to ACIP), the researchers responsible for analyzing the millions of medical records in the CDC’s Vaccine Safety Datalink (VSD) using the ‘Rapid Cycle Analysis’ only studied 23 outcomes. A Similar analysis in NEJM from Israeli researchers focused on only 25 outcomes. Compare this to over 700 safety signals found by the CDC when they finally decided to look—and that’s not even counting all the adverse events that have never been reported for other vaccines so cannot ever show a safety signal by definition. How can the CDC say that these safety signals are meaningless if almost none of them have been studied any further? And yet we are assured that these vaccines have undergone the most intensive safety monitoring effort in history. It’s complete and utter hogwash!
* * *
Josh Guetzkow is a senior lecturer at The Hebrew University of Jerusalem. Subscribe to his Substack here.
1) To be precise, the ‘adverse events’ are for ‘preferred terms’ (PTs) which is a type/level of classification used in the Medical Dictionary for Regulatory Activities (MedDRA), which is the classification system used by VAERS and in other pharmacovigilance systems and clinical research for coding reported adverse events. Not all preferred terms are a symptom or adverse event per se. Some refer to a specific diagnostic test that was done or a treatment that was given.
2) It’s not entirely clear how they divided these up, since there are clearly AEs that should be considered serious that don’t show up in the serious Excel table — though maybe they don’t come up simply because they are looking within serious reports. I believe that they just filtered the reports to include only serious reports or non-serious reports, then did the safety signal analysis on all the AE’s coded in those reports. The reason I think this is that I used the MedAlerts Wayback Machine, selected just the serious COVID-19 vaccine reports, and the numbers of total reports was very close to the one in the table provided by the CDC (MedAlerts actually had a bit less). The files obtained by the Epoch Times do not include much in the way of a description as to how the analyses were done, so I had to infer some details, which might be incorrect. I will try to note when I am drawing an inference about how the analysis was done.
3) Generally speaking, these figures show the top ten AEs in each category. In some cases I combined AEs that indicated the same thing, such as combining ‘heart rate irregular’ with ‘arrythmia.’ [UPDATE: Note that the charts of all categories, cardiac and thrombo-embolic events were updated on Jan 7, 2023. The reason is that I had previously categorized acute myocardial infarction as a cardiac issue and myocardial infarction as thrombo-embolic. To be consistent, I have now combined myocardial infarction and acute myocardial infarction into one AE category in the thrombo-embolic events (which made the total AEs reported for that category larger than for pulmonary ones) and then added a different cardiac AE to the cardiovascular AE category, ventricular extrasystoles, AKA premature ventricular contraction (PVC), which dependent on frequency and the presence of other cardiomyopathies is associated with sudden cardiac arrest.]
4) Note that using the myo-pericarditis signal as a yardstick doesn’t mean that these are the only signals that matter. To give one example, anaphylactic reactions don’t even show up in the list of safety signals, even though that was one of the very first risk of the vaccine that became apparent from day one of the vaccine rollout.
One potential objection to this benchmark is that it is too low of a bar, since myo-pericarditis appears to disproportionately affect younger men and so a proper safety signal should be stratified by age and gender then compared with myocarditis similarly stratified. I agree, and it is the CDC’s job to do that. But the fact is that any adverse reaction might disproportionately affect some subgroup of people, in which case the safety signal for that group would be similarly faint or diluted when we look at everyone together. So objection overruled.
5) In their Standard Operation Procedures document, the CDC said they would combine these and related codes together to assess a safety signal, but never mind – at least they finally got around to doing something.
6) In this context, the Chi-square is largely driven by the sheer number of adverse events: the more adverse events reported, including for the comparator vaccine, the larger the Chi-square. For example, the PRR for pericarditis and subdural haematoma is the same (2.82), but there were 1,701 incidents of pericarditis reported for mRNA COVID vaccines versus 221for the comparator vaccines, with Chi-square of 229.5. For subdural haematoma, these numbers are 162 verus 21, for a Chi-square of 21.2.
GOP Senator Demands DoD Investigate Leaked DARPA Bombshell Over Covid-19 Origins
Sen. Ron Johnson (R-WI) has requested any findings from a Department of Defense investigation into the origins of Covid-19, following the recent publication of a Defense Advanced Research Projects Agency (DARPA) report obtained by Project Veritas.
According to the leaked report written by a Marine, EcoHealth Alliance sought a contract to use controversial gain-of-function genetic manipulation techniques to study bat coronaviruses. While the proposal was rejected by DARPA, it was subsequently picked up by Anthony Fauci’s National Institute of Allergy and Infectious Disease, which funneled money to EcoHealth via a sub-grant.
Fauci has repeatedly claimed NIAID did not fund gain-of-function research into bat coronaviruses.
“It is apparent that Dr. Fauci has not been forthright with the American people regarding his involvement in funding dangerous research,” Sen. Johnson told the Daily Caller.
“According to the Major’s disclosure, EcoHealth Alliance (EcoHealth), in conjunction with the Wuhan Institute of Virology (WIV), submitted a proposal in March 2018 to the Defense Advanced Research Projects Agency (DARPA) regarding SARS-CoVs. The proposal included a program, called DEFUSE, that sought to use a novel chimeric SARS-CoV spike protein to inoculate bats against SARS-CoVs,” reads Johnson’s letter.
“Although DARPA rejected the proposal, the disclosure alleges that EcoHealth ultimately carried out the DEFUSE proposal until April 2020 through the National Institutes of Health and National Institute for Allergy and Infectious Diseases. The disclosure highlights several potential treatments, such as ivermectin, and specifically alleges that the EcoHealth DEFUSE proposal identified chloroquine phosphate (Hydroxychloriquine) and interferon as SARS-CoV inhibitors.”
The leaked documents also suggest that Covid-19 was created at the Wuhan Institute of Virology.
Johnson asks the DoD to interview the Marine who reportedly authored the report, and undertake an investigation into its claims.